Морфология зоны имплантации синтетических герниопротезов, модифицированных углеродом
Морфология зоны имплантации синтетических герниопротезов, модифицированных углеродом

Аннотация
Цель исследования: улучшение исходных свойств биосовместимости синтетических герниопротезов путем модификации поверхности АПП. (DLC-покрытием).
В качестве исходных эндопротезов использовали полипропиленовые сетки (Эсфил легкий) и пленки политетрафторэтиленовые перфорированные пористые (Экофлон). АПП наносили с использованием импульсного источника углеродной плазмы с графитовым катодом. Оперативные вмешательства выполнены в асептических условиях, эндопротезы размерами 1,5×1,5 см помещали подкожно в переднюю брюшную стенку животных вне поля разреза без дополнительной фиксации.
В группе с применением эндопротеза из полипропилена с АПП на 7-е сутки эксперимента вокруг сетчатого протеза определялась равномерная зона грануляционной ткани с визуально меньшей плотностью клеточного состава. На 14-е сутки вокруг протеза с АПП сформировался непрерывный слой грануляционной ткани, было выявлено фрагментирование покрытия в виде пластинчатых и игольчатых фрагментов. Через 180 суток имела место морфологическая картина полной инкапсуляции материала сформированной капсулой, структурно полностью интегрированной в окружающую соединительную ткань. Острой воспалительной и гигантоклеточной реакции на фрагменты покрытия не было выявлено. В группе с эндопротезом из политетрафторэтилена на 7-е и 14-е сутки острые воспалительные изменения отсутствовали. Через 180 суток установлены отличительные особенности в виде выраженных депозитов адгезивных белков (фибронектина и ламинина) и коллагена I типа, слой покрытия сохраняется и не подвергается механическому разрушению. В прилежащей соединительной ткани не выявлено воспалительной реакции.
Сетчатые эндопротезы полипропилен и политетрафторэтилен с АПП обладают большей биосовместимостью и лучшей биоинтеграцией в окружающие ткани в процессе инкапсуляции в отдаленные сроки, в сравнении с исходными материалами.
1. Introduction
Currently, there is a steady increase in the number of reconstructive and restorative surgical interventions using biomaterials in various fields of surgery. At the same time, many authors note unresolved issues regarding the biocompatibility of surgical endoprostheses implanted into the body. This is due to the fact that during the integration of synthetic material with body tissues, a response occurs in the form of aseptic inflammation, resulting in the formation of a connective tissue capsule, which can lead to tumor development, implant calcification, infection, and prosthesis dysfunction .
These complications lead to impaired function of synthetic prostheses, causing deterioration in the patient's health and requiring repeat interventions.
Reducing the risk of complications is currently achieved through two main approaches: modifying the structure of the synthetic implant itself and applying various coatings.
DLC coating (nanoscale diamond-like carbon coating — APP) is an amorphous carbon-based film containing mixed sp3 and sp2 carbon-carbon bonds. Currently, this coating is used as a polymer coating for various medical devices (mesh implants, stents, and prostheses for cardiovascular surgeries, endoprostheses in trauma operations). However, it has not gained wide application in surgical practice, as its application requires special expensive equipment and due to the complexity of the technology for applying it to various synthetic coatings.
The method developed at NIU "BelSU" allows applying APP to synthetic materials, which can also be used for closing soft tissue defects (Patent No. 2430986).
Thus, the aim of our study is to investigate the main biocompatibility properties of synthetic hernioplasty endoprostheses whose surfaces are modified with APP.
2. Research methods and principles
The fabrication of original endoprostheses with carbon coating was carried out at NIU "BelSU." Polypropylene mesh endoprostheses Esfil Light (Lintex, Russia) and perforated porous polytetrafluoroethylene films Ecoflon (Ecoflon, Russia) were used as base implants.
APP was applied to these samples using a pulsed carbon plasma source with a graphite cathode under the following parameters: capacitor capacity — 2300 μF, capacitor charging voltage — 300 V, pulse discharge frequency 1–2 Hz.
Animal studies were conducted at the Laboratory of the Research Institute of "Pharmacology of Living Systems" at NIU "BelSU" (Director: Doctor of Medical Sciences, Professor M.V. Pokrovsky). The work was performed in accordance with the approved research protocol and standard laboratory operating procedures. All stages complied with the Russian National Standard GOST R-53434-2009 "Principles of Good Laboratory Practice," the Order of the Ministry of Health and Social Development of the Russian Federation dated August 23, 2010, No. 708n "On Approval of Laboratory Practice Rules," in compliance with the interstate standard "Guidelines for the Care and Use of Laboratory Animals" (GOST 33216-2014), and ethical principles concerning laboratory animals following the European Convention for the Protection of Vertebrate Animals Used for Experimental and Other Scientific Purposes CETS No. 123, as amended by ETS No. 170.
The study involved 220 male Wistar rats weighing 200 g.
In the experimental study, animals were divided into a group using polypropylene prostheses (n=120) with coating (n=60) and without coating (n=60), and a group using polytetrafluoroethylene prostheses (n=100) with coating (n=50) and without coating (n=50).
Surgical interventions were performed under aseptic conditions. After preparing the surgical field, experimental endoprostheses sized 1.5×1.5 cm were implanted subcutaneously into the anterior abdominal wall outside the incision field without additional fixation. The wound was sutured. Animals were withdrawn from the experiment on days 7, 14, and 180.
Histological specimens were scanned using the "Mirax Desk" system (Carl Zeiss) for scanning, archiving, and image analysis. Specimens were stained with hematoxylin and eosin according to Van Gieson and Mallory methods.
Microscopic images and morphometry were analyzed on scanned micropreparations using the "Pannoramic Viewer 1.14" software. Microphotographs were captured using the same software and with "Fast Stone Capture" image capture software.
Statistical significance between groups was assessed using the Mann–Whitney test. The calculation of the test statistic and p-value was performed with the Statistica 12.5 statistical software package. At p < 0.05, the null hypothesis (H₀) of equal means is rejected, and the alternative hypothesis of statistically significant differences between compared groups is accepted.
3. Main results
Morphology of the implantation zone of polypropylene and polytetrafluoroethylene hernioplasty prostheses without coating. Upon implantation of both materials up to 180 days, no signs of damaging toxic effects on subcutaneous tissues were detected. The observed tissue reactions reflect the typical sequence of changes in the foreign body implantation zone characteristic for each material.
Implantation of uncoated polypropylene mesh was characterized by long-lasting inflammatory changes — in day 14 samples, granulation tissue with signs of incomplete maturity and foci of inflammatory reaction were observed, persisting even after 6 months (Fig. 1).
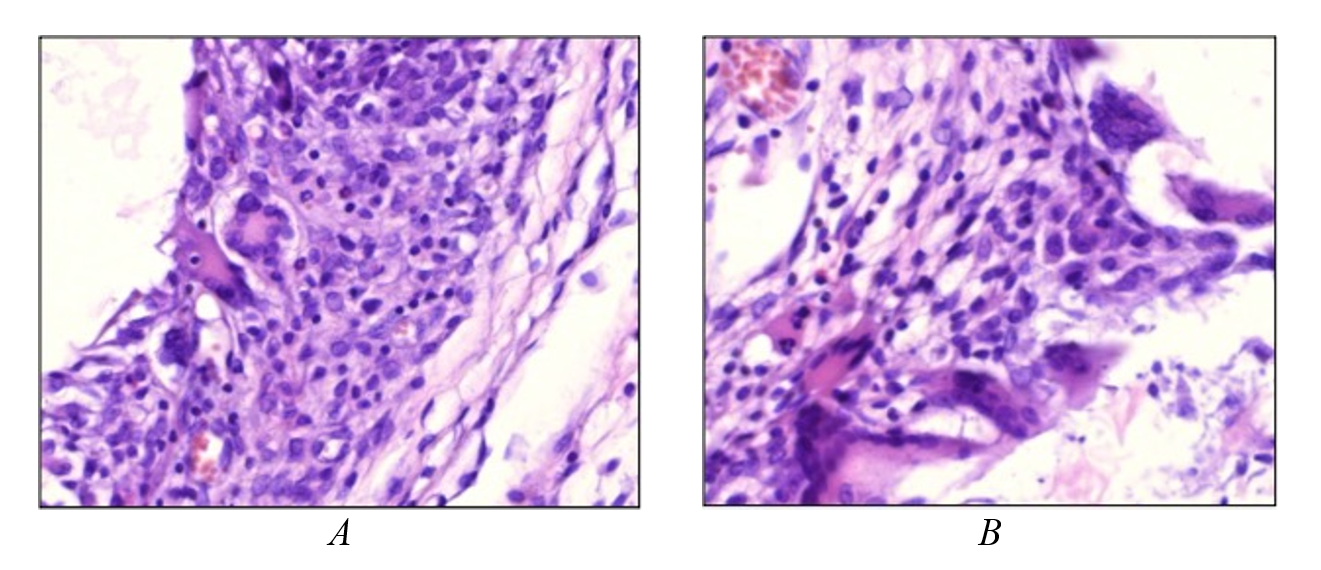
Figure 1 - Implantation area of polypropylene hernioplasty meshes without coating:
A – structure of granulation tissue around the uncoated polypropylene implant on day 14 of the experiment: mixed polymorphic cellular composition with a predominance of leukocytes and histiocytes, presence of multinucleated foreign body giant cells; B – numerous giant multinucleated foreign body cells around the implant on day 14 of the experiment
Note: stained with hematoxylin and eosin; microphoto. ×400
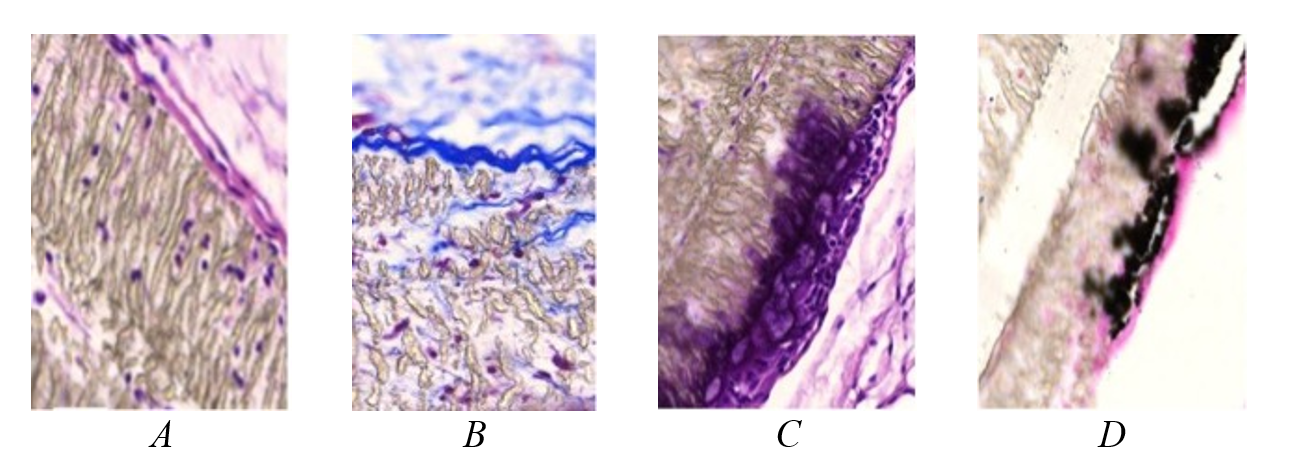
Figure 2 - 180 days after implantation of an uncoated polytetrafluoroethylene plate:
A – the implant structure is moderately loosened; on the outside, single loosened collagen fibers of the connective tissue of the anterior abdominal wall1; B – leukocyte migration into the pores of the material, ingrowth of single thin collagen fibers2; C – giant foreign body cell layer3; D – area of calcification in the region of foreign body cell accumulation4
Note: 1 – stained with hematoxylin and eosin; microphoto. ×100; 2 – mallory staining; microphoto. ×200; 3 – stained with hematoxylin and eosin; microphoto. ×100; 4 – kossa impregnation; microphoto. ×100
The common response to implantation of both materials was the formation of a characteristic connective tissue capsule after 180 days. On the surface of the polypropylene mesh, formed connective tissue appeared as a heterogeneous capsule 80–100 μm thick, with prevalently concentrically organized dense fibrous, focally hyalinized connective tissue with few fibrocyte-type cells (Fig. 1). However, up to one-third of the encapsulating connective tissue area, especially in regions of implant element intertwining, showed moderate leukocyte infiltration with significant eosinophil content. These areas also contained a moderate number of blood capillaries. Foreign body cells were absent, but epithelioid histiocyte plates were segmentally arranged on the inner capsule surface. There was no full integration of capsule structures into the surrounding connective tissue — a distinct boundary was visible.
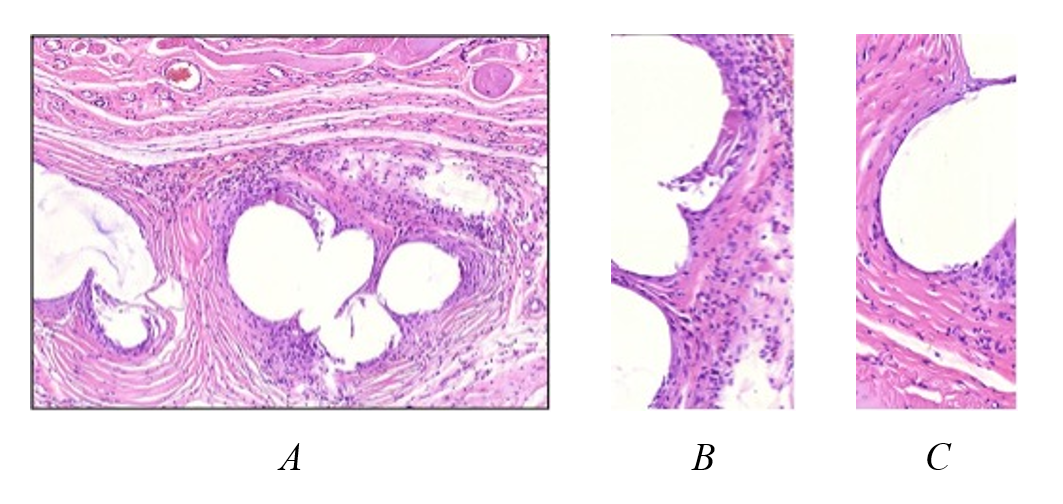
Figure 3 - Structure of the capsule of an uncoated polypropylene implant after 6 months:
the connective tissue is heterogeneous, with predominance of areas of dense fibrous structure (C) containing few fibrocyte-like cells; up to one-third of the area consists of regions with pronounced infiltration by polymorphonuclear leukocytes, predominantly eosinophils (B); foreign body cells are absent, but epithelioid histiocyte-like cells are present on the inner surface of the capsule
Note: stained with hematoxylin and eosin; microphoto. ×20 (A), ×400 (B, C)
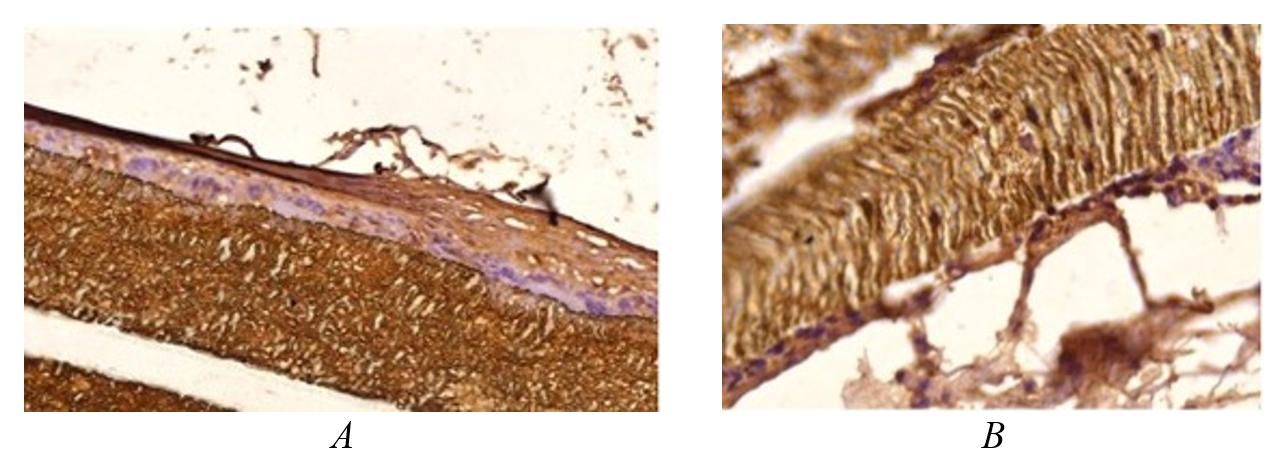
Figure 4 - Deposits of fibronectin (A) and type I collagen (B) in the bulk and on the surface of an uncoated polytetrafluoroethylene implant
Note: immunohistochemical reactions; microphoto. ×100
The overall implantation picture of polypropylene with carbon coating showed complete material encapsulation with a capsule fully integrated structurally into the surrounding connective tissue (Fig. 5).
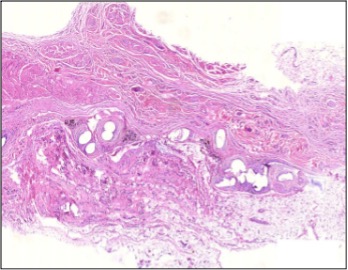
Figure 5 - Overall view of the implantation area of carbon-coated polypropylene mesh after 6 months of the experiment.
Note: A continuous layer of connective tissue surrounds the implant without clear boundaries from the surrounding tissues. Stained with hematoxylin and eosin. Microphoto. ×20.
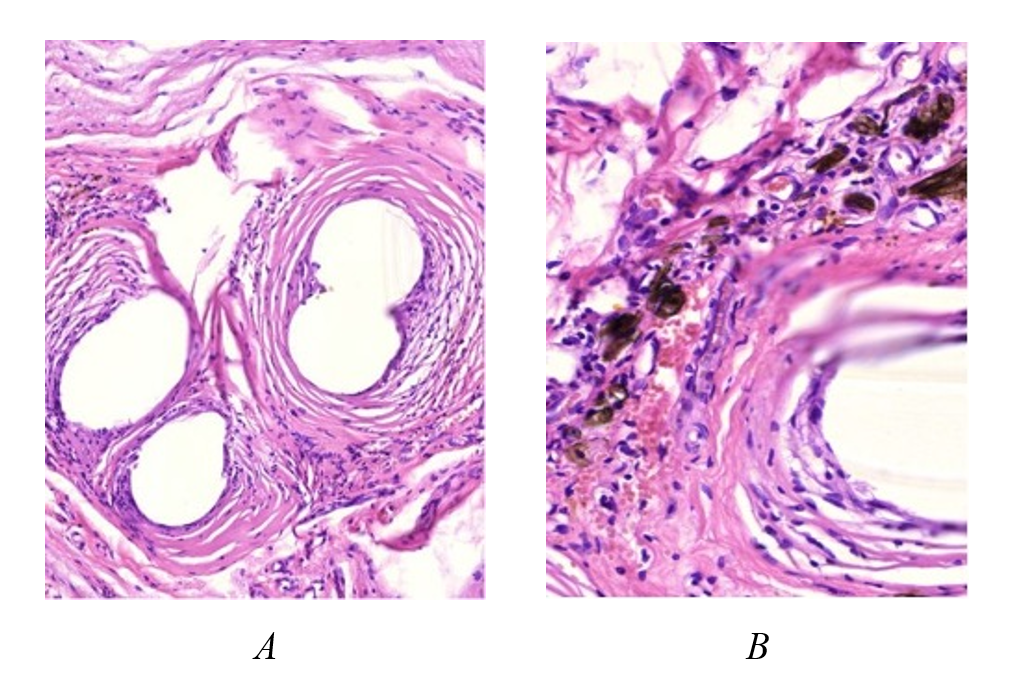
Figure 6 - Structure of the connective tissue capsule around the polypropylene mesh:
A – concentric low-cell-density layers of collagen fibers with a smooth transition into the surrounding connective tissue, absence of inflammatory changes and giant cell reaction to the implant; B – plate-like and needle-like coating particles in close proximity to the implant, surrounded by vascularized loose fibrous connective tissue with a moderate number of lymphohistiocytic elements
Note: stained with hematoxylin and eosin; microphoto. ×20 (A), ×400 (B)
On the surface of polytetrafluoroethylene, 180 days after implantation, the carbon layer in histological specimens showed no mechanical damage, indicating strong fixation (Fig. 7). No significant inflammatory changes were observed in adjacent connective tissue, and mast cells were intact. No calcification foci were detected. The overall picture suggested reduced implant porosity and permeability for inflammatory elements and intercellular substance components, including growing collagen fibers. Implant encapsulation occurred without connective tissue ingrowth, via capsule formation with a more external location and broad tissue delimitation around the implant.
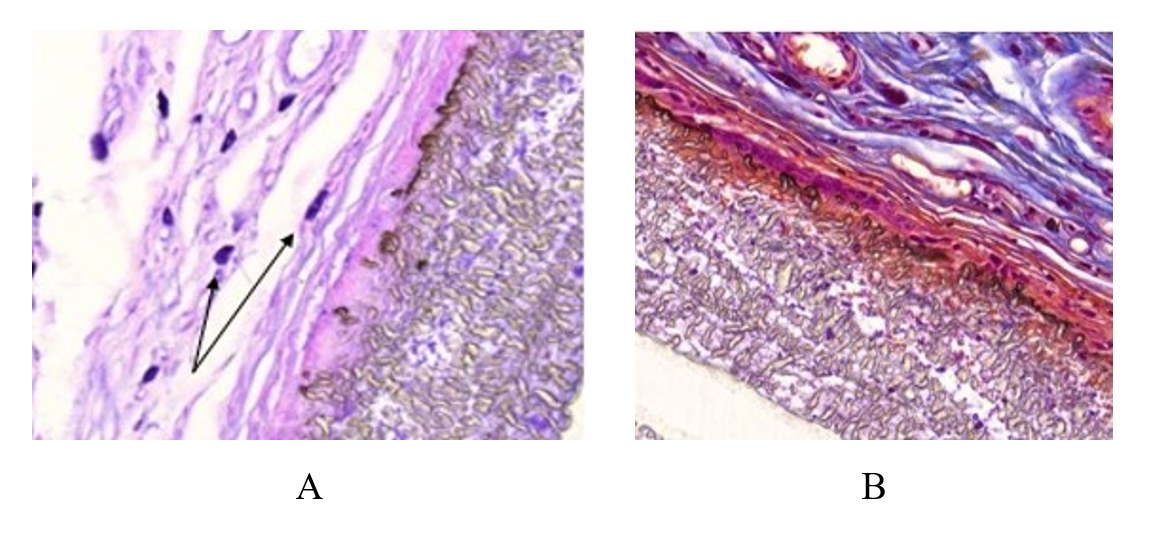
Figure 7 - 180 days after implantation of a polytetrafluoroethylene plate with a carbon coating:
A – tight adhesion of the implant to the connective tissue, the carbon coating layer is preserved as a narrow brown stripe; intact mast cells are indicated by arrows; B – section of the implant surface showing layers of immature collagen fibers of the forming capsule and surrounding abdominal wall tissues with bundles of mature collagen fibers (blue color); connective tissue does not grow into the thickness of the implant; between the capsule fibers and the implant surface, there are few small foreign body cells
Note: stained with Phenaf dye (A), mallory staining (B); Microphoto.×100
Table 1 - Study group "Ecoflon," Subgroups with Coating and without Coating
| Groups | Observation periods | Reliability of differences | ||
Day 7 | Day 14 | 180th day | |||
Infiltrate thickness, µm | Control | 175±25 | - | - | P1*=0.04 P2*>>0.05 P3*>>0.05 |
With coating | 125±25 | - | - | ||
Polymorphonuclear leukocytes,% | Control | 52±8 | 30±5 | - | P1*<<0.01 P2*=0.01 P3*>>0.05 |
With coating | - | 12±3 | - | ||
Small lymphocyte type cells,% | Control | 22±3 | 17±3 | - | P1*<<0.01 P2*=0.08 P3*<<0.01 |
With coating | - | 12±3 | 9±1 | ||
Histiocytes,% | Control | 22±3 | 30±2 | 40±4 | P1*=0.02 P2*=0.01 P3*<<0.01 |
With coating | 37±7 | 7±1 | - | ||
Foreign body giant multinucleated cells (FBGCs) | Control | 3±2 | 10±1 | - | P1*<<0.01 P2*<<0.01 P3*<<0.01 |
With coating | - | - | - | ||
Capsule thickness, µm | Control | - | 200±30 | 90±10 | P1*>>0.05 P2*=0.04 P3*=0.02 |
With coating | - | 147±22 | 55±5 | ||
P1*- valuep-value for the group indicator on day 7;P2*- valuep-value for the group indicator on day 14;P3*- valuep-value for the group indicator at day 180;
Table 2 - Study group "Esfil-light," Subgroups with Coating and without Coating
| Groups | Observation periods | Reliability of differences | ||
Day 7 | Day 14 | 180th day | |||
Infiltrate thickness, µm | Control | 125±25 | - | - | P1*=0.04 P2*>>0.05 P3*>>0.05 |
With coating | 90±10 | - | - | ||
Polymorphonuclear leukocytes,% | Control | 47±3 | 25±4 | - | P1*=0.1 P2*=0.04 P3*>>0.05 |
With coating | 42±3 | 17±3 | - | ||
Small lymphocyte type cells,% | Control | 20±2 | 15 ± 2 | - | P1*=0.1 P2*=0.04 P3*<<0.01 |
With coating | 17 ± 2 | 10 ± 1 | 7±1 | ||
Histiocytes,% | Control | 26±2 | 27±2 | 35 ± 3 | P1*=0.08 P2*=0.02 P3*=0.004 |
With coating | 22±2 | 17 ± 2 | 10 ± 2 | ||
Foreign body giant multinucleated cells (FBGCs) | Control | 7±1 | 9±1 | - | P1*<<0.01 P2*<<0.01 P3*<<0.01 |
With coating | - | - | - | ||
Capsule thickness, µm | Control | - | 175±35 | 70±10 | P1*>>0.05 P2*=0.05 P3*=0.03 |
With coating | - | 130±10 | 52±5 | ||
P1*- valuep-value for the group indicator on day 7;P2*- valuep-value for the group indicator on day 14;P3*- valuep-value for the group indicator at day 180.
4. Discussion
Modern surgical endoprostheses for hernioplasty are predominantly made from non-resorbable synthetic materials, including polypropylene and polytetrafluoroethylene. Despite the achieved reduction in recurrence rates, the persistent risk of specific postoperative complications indicates insufficient effectiveness of current technologies, necessitating further research and development in this area. Current studies focus on developing endoprostheses capable of mimicking native tissue and promoting healing without postoperative complications. Researchers actively investigate advanced biodegradable materials, both synthetic polymers and natural biopolymers, as well as the efficacy of therapeutic agents, surface modification methods, and advanced manufacturing technologies such as 4D printing. Our work is specifically aimed at modifying the surface of materials used for hernia repair by applying a novel diamond-like carbon coating developed at NIU "BelSU" and evaluating its use.
Upon implantation of polypropylene with carbon coating, significant differences were observed as early as day 7, manifested by earlier formation of the fibroblastic component in granulation tissue, as reflected by the relative count of cellular elements in infiltrates. By day 14, fibroblasts with morphological features of functionally active forms and zones of amorphous and fibrous intercellular substance formation were clearly observed. At late time points (6 months), full biointegration of the implant into subcutaneous connective tissue was identified as reactive encapsulation by connective tissue directly connected with surrounding structures. No inflammatory or other reactive changes were noted.
At the same time, disintegration of the implant’s surface coating was clearly observed. Its fragments were compactly deposited nearby and surrounded by loose connective tissue. However, no signs of inflammatory reaction or typical foreign body responses were detected, allowing us to classify the coating particles as bioinert. The implant surface at this stage was open, but surrounded by a formed, practically avascular dense fibrous tissue. The avascularity of the formed fibrous capsule determines its areactivity. It can be assumed that the duration of intactness of the fully bioinert coating is sufficient for the formation of the areactive capsule, and subsequent coating disintegration no longer plays a role given the established biointegration of the implant. This is indicated by comparison of the morphological pictures at late stages for implants without coating and with coating.
A somewhat different picture emerged after implantation of polytetrafluoroethylene with carbon coating. The original microporous polytetrafluoroethylene implant absorbed plasma and matrix proteins and was subsequently infiltrated by collagen fibers, which could cause rigid fixation of the implant to the anterior abdominal wall tissues. A negative consequence of this was mechanical impact of implant edges on tissues, manifested as calcification foci with giant cell reaction in these areas. Surface modification of polytetrafluoroethylene plate implants by nanoscale diamond-like carbon coating improved their properties by eliminating microporosity and preventing infiltration of connective tissue components and protein exudation, including inflammatory reaction components, thereby reducing connective tissue fiber ingrowth and the degree of secondary calcification.
One of the most significant differences in tissue reactions to carbon surface modification of synthetic prostheses was the absence, at all time points, of macrophage giant cell transformation and foreign body cell formation. In current literature, the response of the mononuclear phagocyte system, including giant cell formation, is regarded as a key indicator of implant biocompatibility. However, the dependence of these processes on the physico-chemical surface characteristics of implant materials remains under discussion. Shen M. et al. demonstrated that adsorbed proteins and surface chemical composition strongly influence giant cell formation, monocyte TNF-alpha release, and procoagulant activity in vitro, supporting the idea that these variables may also affect macrophage-mediated foreign body response to biomaterials in vivo.
Surface modification of biomaterials determines their interaction with cells, including adhesion and programmed cell death processes. Notably, implant surface-induced apoptosis of immunocompetent cells (monocytes/macrophages) may create conditions for persistence of infectious agents, supported by clinical data on cardiovascular implants.
Our study established that the most pronounced giant cell reaction occurred with implantation of non-modified materials, accompanied by accumulation of fibronectin and type IV collagen. Use of the specialized coating significantly reduced the intensity of this cellular response.
Several explanations for this difference exist, yet literature data do not provide a definitive conclusion, since calcification signs were observed in tissue zones in direct contact with implant surfaces in giant cell reaction areas.
Critically, the created coating modulates tissue response to the implant, defining two possible scenarios: full biomechanical integration by connective tissue incorporation or formation of a connective tissue capsule as a manifestation of foreign body rejection. Further studies on implant biodegradation kinetics depending on surface modification types should be promising.
5. Conclusion
The obtained data indicate that synthetic implants with nanoscale diamond-like carbon surface modification, compared to the original materials, possess higher biocompatibility and better biointegration into surrounding connective tissue during late-stage encapsulation.
The developed technology for applying coatings with specified properties to polymer implants is an effective method for controlling implant characteristics depending on the desired application outcome. Based on these results, a clinical study is needed to investigate the interaction of DLC-покрытия with the human anterior abdominal wall.