SUCCESSFUL TREATMENT OF COMPLICATED CHRONIC POST-TRAUMATIC TIBIAL OSTEOMYELITIS (A CLINICAL CASE REPORT)
SUCCESSFUL TREATMENT OF COMPLICATED CHRONIC POST-TRAUMATIC TIBIAL OSTEOMYELITIS (A CLINICAL CASE REPORT)
Abstract
In the article, the authors describe a successful clinical case of treating chronic post-traumatic osteomyelitis of the tibia in a 43-year-old patient with non-union fracture and deep trophic shin ulcer. The team applied a combined surgical approach, which included segmental resection of the affected bone segment with external fixation, as well as soft tissue defect repair using a non-free skin-subcutaneous-fascial flap. Postoperative management involved antibacterial therapy, anticoagulant and antiplatelet support, and step-by-step rehabilitation. In the long-term follow-up, the patient achieved complete fracture union, absence of the infection recurrence, and restoration of limb weight-bearing function. This method proves effectiveness in complicated chronic osteomyelitis treatment in areas with soft tissue deficiency and may be recommended for clinical use.
1. Introduction
Osteomyelitis is a widespread disease, accounting for up to 6% of musculoskeletal disorders and 7–12% of surgical infections , . In cases of open bone fractures, it develops in 5.3–75.4% of patients, and in 7.6–33.2% of cases — following surgical treatment of closed fractures and orthopedic bone procedures . Among purulent surgical infections, osteomyelitis holds a leading position due to its high prevalence, severe clinical course, diagnostic and therapeutic challenges, and a significant rate of diverse complications. Moreover, it represents a major socioeconomic burden, as up to 78% of patients are of working age (20–50 years), and this group exhibits the highest rate of disability (over 70%) , .
The treatment of chronic osteomyelitis remains one of the most challenging problems in modern surgery . Currently, the standard approach — regardless of etiology, pathogenesis, or lesion localization, involves a two-stage surgical procedure. The first stage entails radical surgical debridement and adequate drainage of the purulent-necrotic focus, while the second stage focuses on eliminating residual bone cavities and soft tissue defects , .
The problem of bone defect reconstruction becomes most critical when the pathological focus is located in the distal shin and proximal foot regions. The soft tissue deficiency in these lower limb segments prevents the use of mobilized local tissues for bone cavity reconstruction and significantly limits the application of antibiotic-loaded methylmethacrylate spacers, which require adequate soft tissue coverage .
Effective soft tissue defect reconstruction necessitates the use of tissue complexes that most closely match the anatomical and functional characteristics of the lost tissues. In such cases, optimal clinical outcomes can be achieved by utilizing tissues from adjacent areas that share similar properties with the defect-surrounding integumentary structures .
This clinical observation makes the authors' following case report of particular professional interest.
2. Clinical Case Report
Patient Yu., 43 years old male, was admitted to Surgical Department No. 2 of the Propaedeutic Surgery Clinic at Samara State Medical University (hereinafter — SamSMU) on January 30, 2023, with a diagnosis of "Non-union fracture of the left tibia. Chronic post-traumatic osteomyelitis of the left tibia. Deep (bony) post-traumatic trophic ulcer of the left shin". The diagnosis and clinical presentation corresponded to type IV of the Cierny–Mader classification of osteomyelitis , while the trophic ulcer matched a medium-sized defect and grade III depth according to Obolensky .
Upon admission, the patient complained of:
· a non-healing skin and soft tissue defect in the middle third of the anterior surface of the left shin with scanty purulent discharge;
· moderate pain in the affected area;
· lack of weight-bearing capacity in the left lower limb.
Medical history revealed that in June 2022, the patient sustained a comminuted fracture of both bones of the left shin due to a traffic accident. Emergency care providers transported him to the trauma department of a district hospital, where surgeons urgently performed open reduction and extra-cortical fixation of the tibia and fibula using plate osteosynthesis. In the postoperative period, an infectious complication developed at the surgical site, which required surgical debridement. Follow-up radiographic examination showed no signs of fracture consolidation.
In September 2022, the patient was readmitted to the same hospital due to the formation of a chronic wound with purulent discharge at the surgical site. Surgeons performed wound debridement supplemented by osteoperforation of the tibia. Radiography of the injured area showed no signs of tibial fracture consolidation. In the postoperative period, purulent discharge from the wound persisted.
By November 2022, doctors removed the bone plates and performed osteonecrectomy of the tibia. However, the shin wound failed to heal, and local post-traumatic trophic disorders developed in the surrounding soft tissues.
As part of scheduled care, the patient was referred for consultation at the SamSMU Clinics. Following evaluation, physicians established the diagnosis: "Non-union fracture of the left tibia. Chronic post-traumatic osteomyelitis of the left tibia. Deep (bony) post-traumatic trophic ulcer of the left shin". The medical team recommended subsequent hospitalization for radical treatment of chronic osteomyelitis.
On admission to SamSMU Clinics, the patient's general condition was satisfactory. Body temperature measured 36.7°C. Physical examination revealed no pathological changes in organ systems. The patient ambulated exclusively using crutches without bearing weight on the left lower extremity.
Laboratory findings demonstrated the following profile.
Complete blood count:
Erythrocytes: 3.89 × 10¹²/L
Hemoglobin: 136 g/L
Platelets: 379 × 10⁹/L
Leukocytes: 8.6 × 10⁹/L (band neutrophils: 2%, segmented neutrophils: 56%, lymphocytes: 28%, monocytes: 4%)
Erythrocyte Sedimentation Rate (ESR): 26 mm/h
Biochemical analysis:
Total protein: 85.8 g/L
Urea: 7.8 mmol/L
Creatinine: 110 μmol/L
Glucose: 4.5 mmol/L
Coagulation profile:
Activated Partial Thromboplastin Time (aPTT): 26.8 sec
International Normalisation Ratio (INR): 1.23
Prothrombin time: 10.3 sec
Quick's prothrombin activity: 64%
The left shin showed no edema or erythema. On the anterior surface of its middle third, there was a 6 × 2 cm skin and soft tissue defect with scanty purulent discharge. The base of the defect consisted of ulcerated grayish tibial bone with multiple osteoperforation fenestra (Figure 1a). Pathological mobility of the shin was evident in the area of the trophic ulcer. Range of motion in the joints of the left lower extremity remained intact, with preserved sensation. Peripheral pulses (dorsalis pedis, popliteal, and femoral arteries) were palpable. No signs of venous insufficiency were detected.
Microbiological examination of the wound discharge revealed Staphylococcus aureus with a concentration of 106 microbial cells, sensitive to ceftriaxone, ampicillin-clavulanate, amikacin, levofloxacin, and ciprofloxacin.
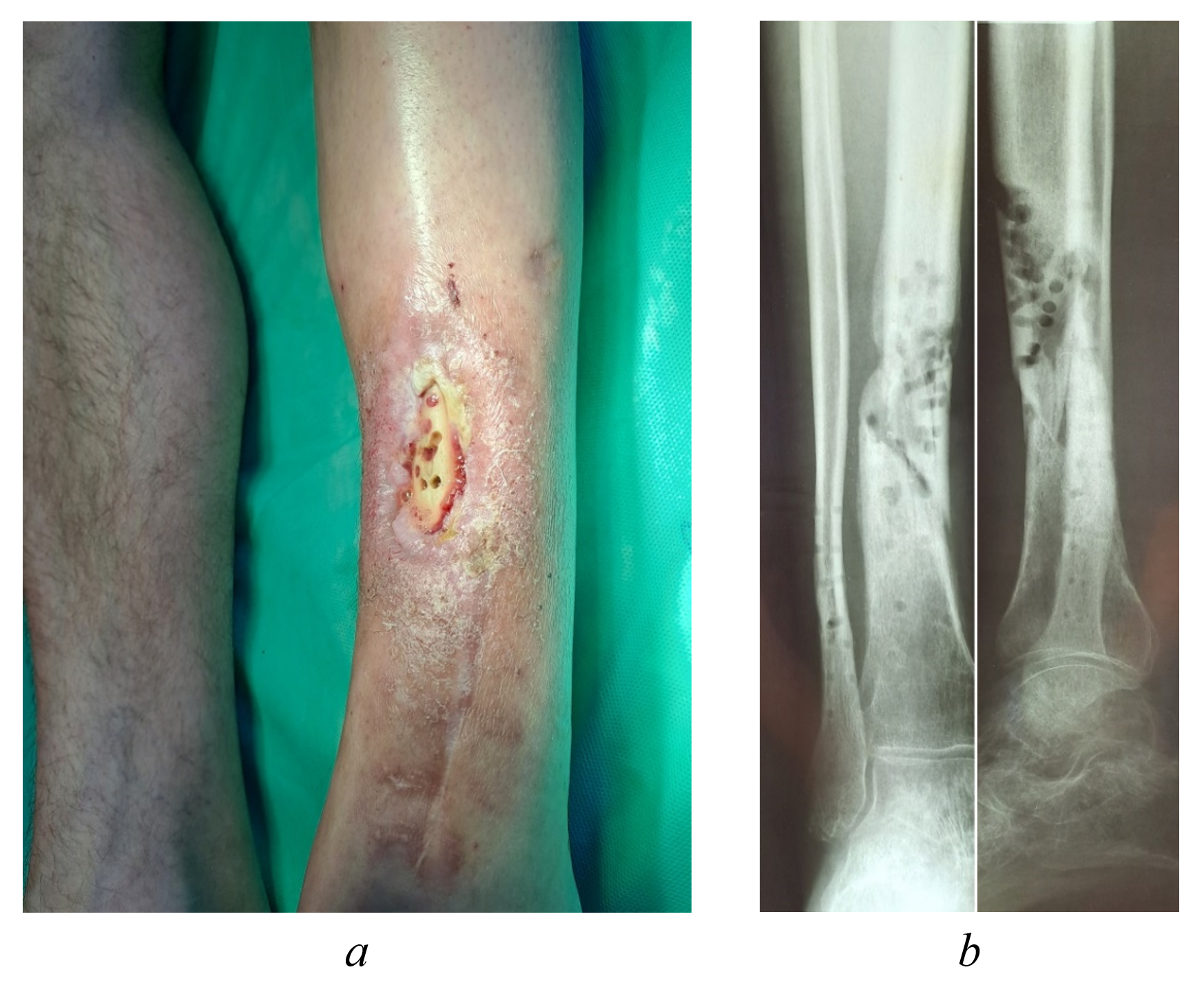
Figure 1 - External appearance (a) and radiograph (b) of the left shin of patient Yu., 43 years old, upon admission to the Clinics of SamSMU
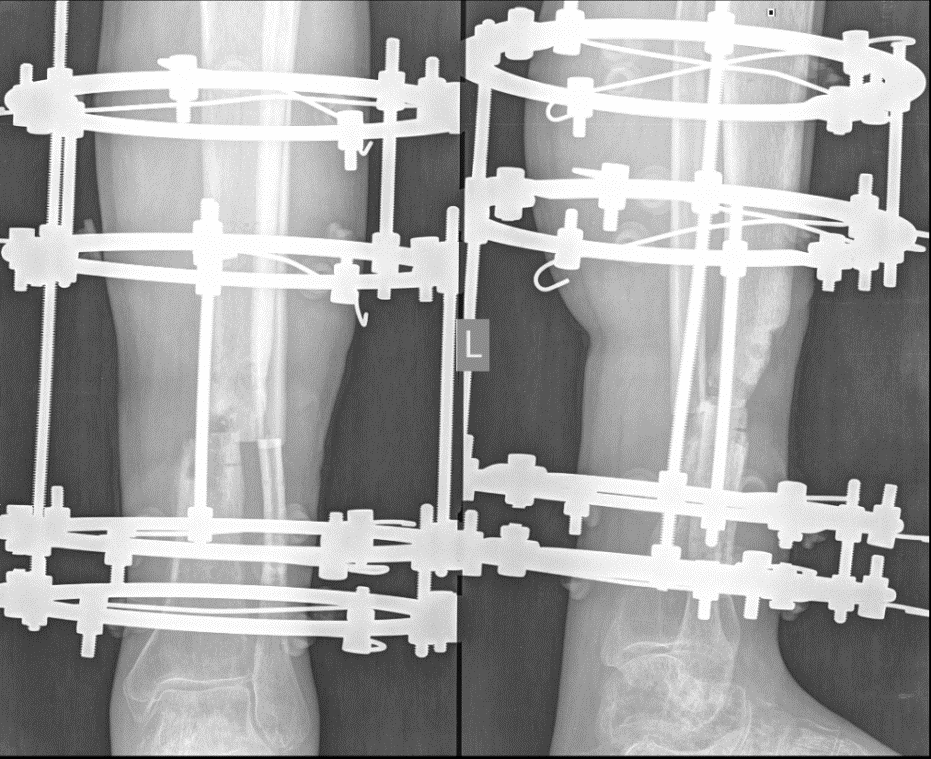
Figure 2 - Intraoperative radiograph of the left shin of patient Yu., 43 years old

Figure 3 - Surgical stage - formation of a pedicled skin-subcutaneous-fascial flap for wound closure

Figure 4 - Postoperative appearance of the left shin in patient Yu., 43 years old, on day 7 after surgery
The patient was discharged on February 14, 2023 with the following recommendations: povidone-iodine wound dressings until complete wound healing (epithelialization), static weight-bearing on the left lower limb in corrective footwear one month after surgery, and follow-up examination three months postoperatively. Following discharge, the patient received outpatient care. He gradually began ambulating with weight-bearing on the left lower limb using corrective footwear. The left leg shortening measured 4 cm.
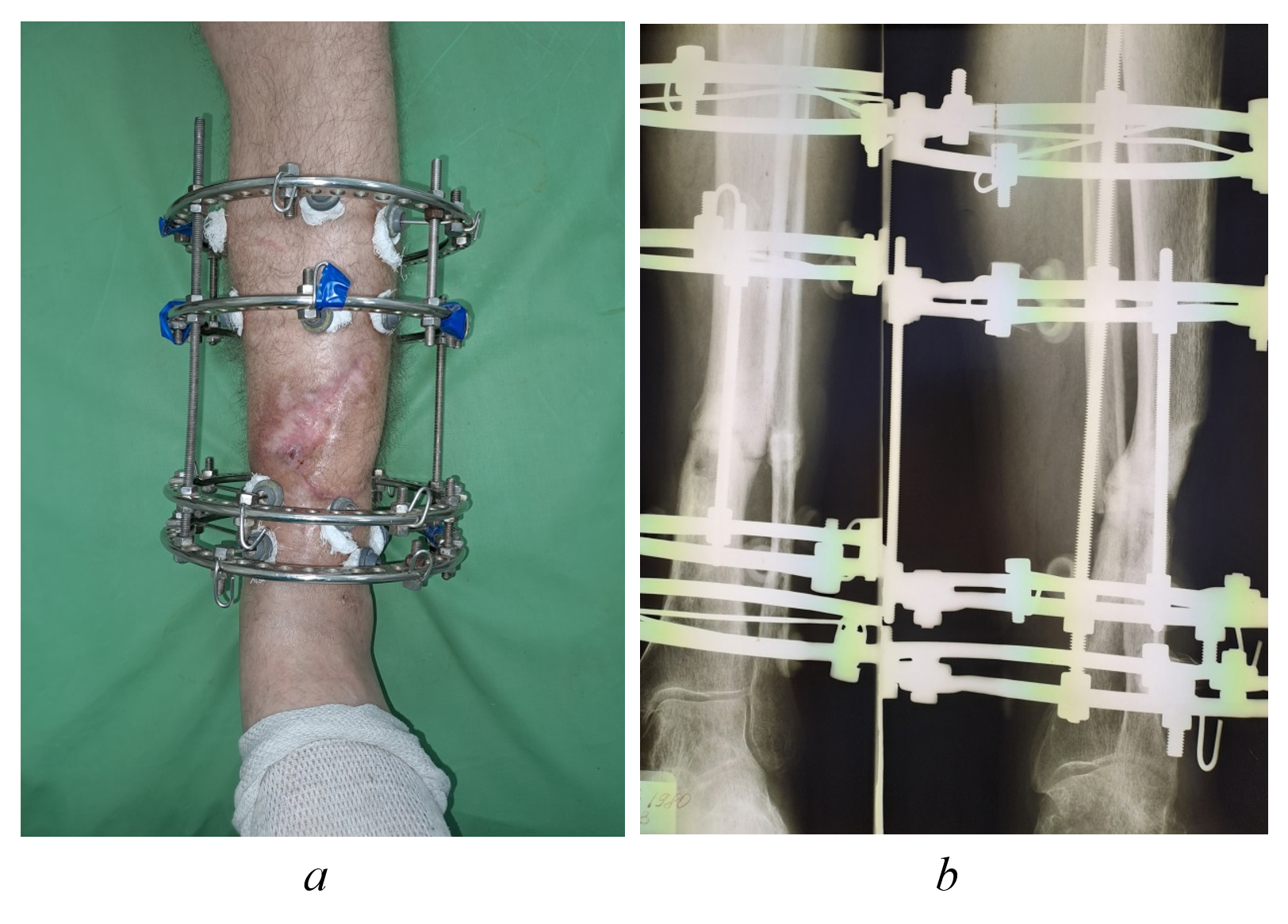
Figure 5 - Clinical appearance (a) and radiographic image (b) of the left shin in patient Yu., 43 years old, at 5-month postoperative follow-up
On September 7, 2023, the patient underwent scheduled surgical removal of the external fixation device. The postoperative course was uncomplicated. The medical team discharged the patient on September 11, 2023 with the following recommendations: continuation of treatment in the medical rehabilitation department, gradual increase of weight-bearing on the left lower limb, and ambulation with corrective orthopedic footwear.
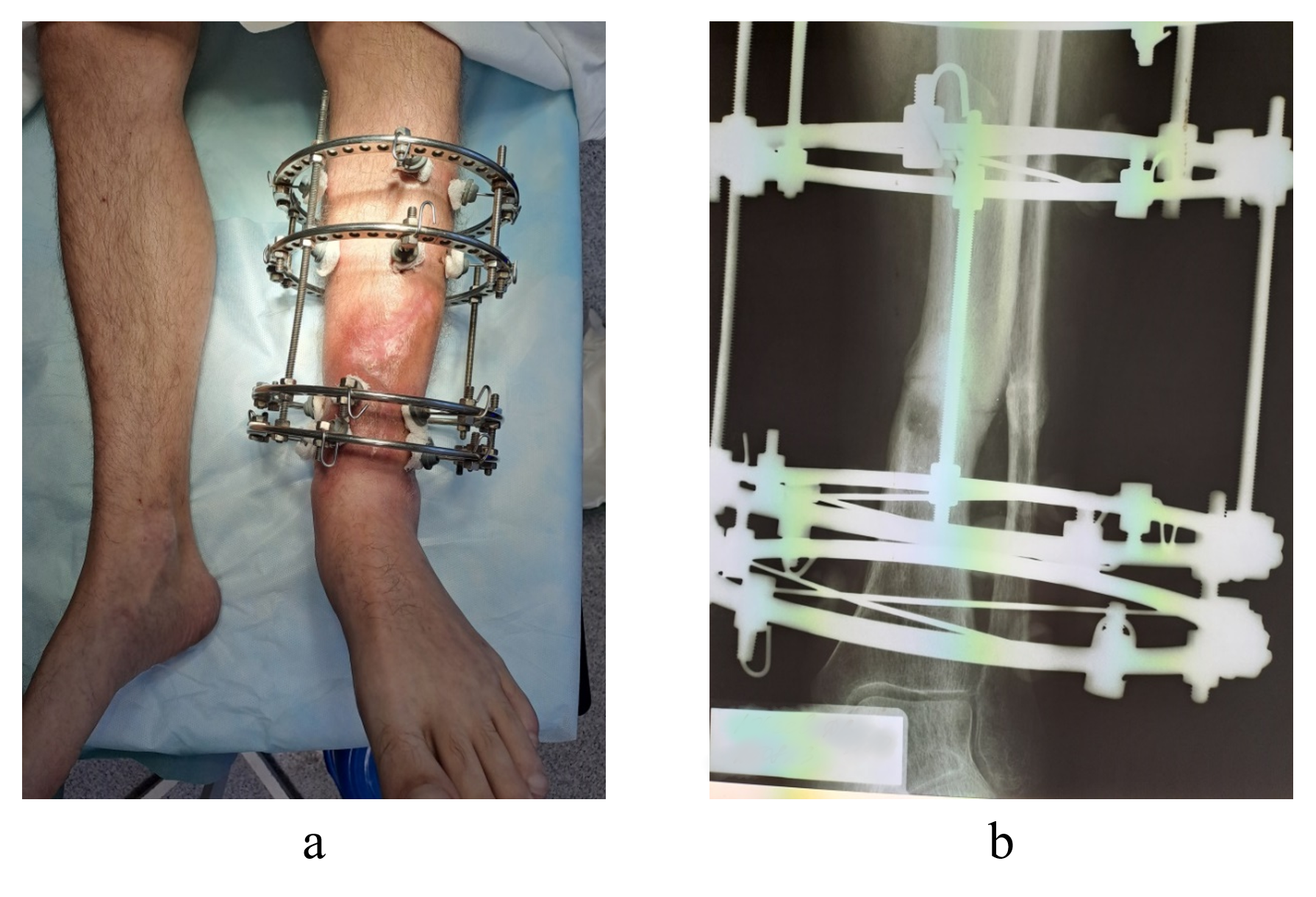
Figure 6 - Clinical appearance (a) and radiographic findings (b) of the left shin in patient Yu., 43 years old, at 7-month postoperative follow-up
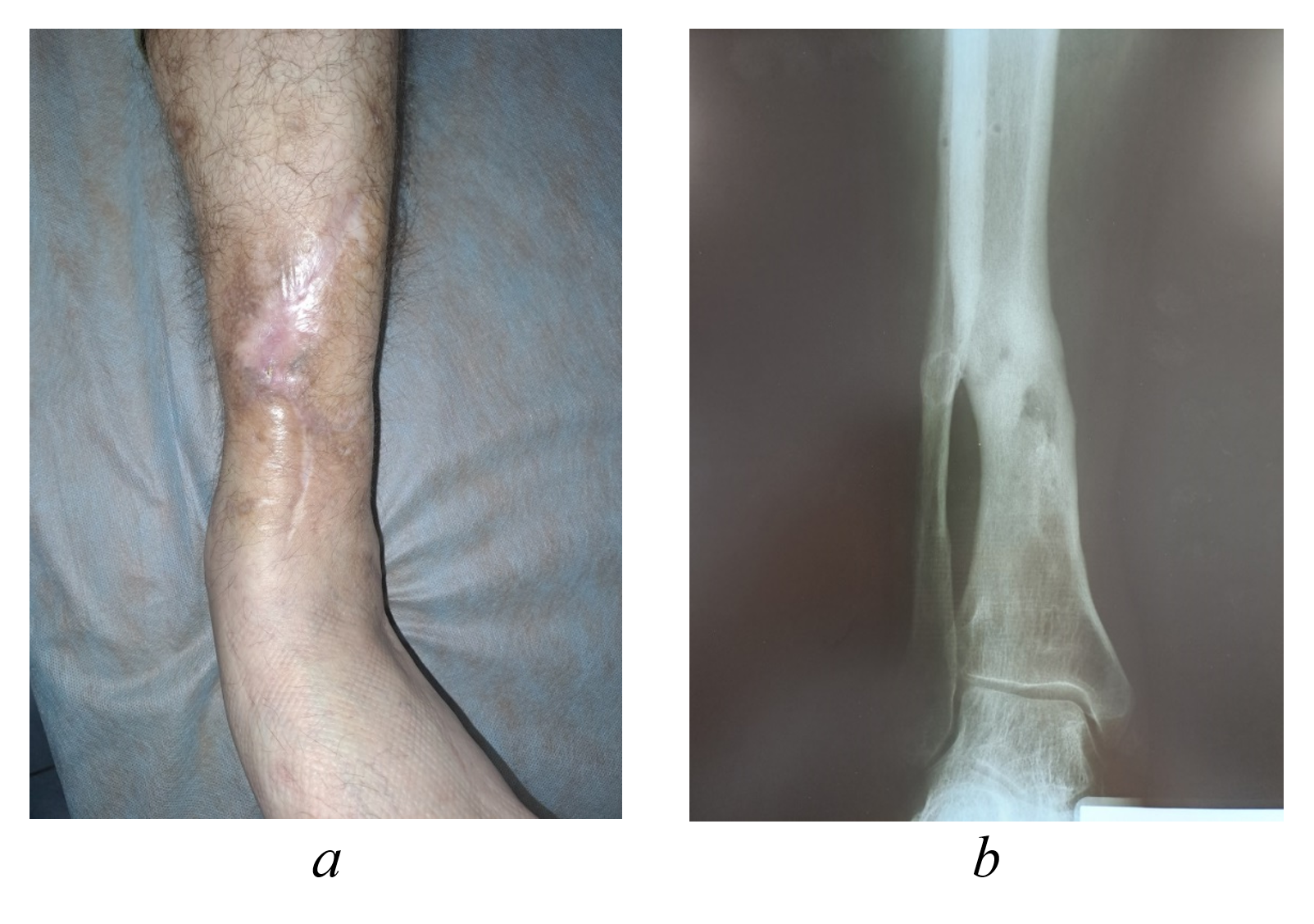
Figure 7 - Clinical appearance (a) and radiographic imaging (b) of the left shin in patient Yu., 43 years old, at 13-month postoperative follow-up
3. Discussion
This case analysis enables evaluation and comparison of the treatment approach's effectiveness with similar clinical cases and published research on chronic osteomyelitis management, particularly in cases with regional soft tissue deficiency and associated complications.
First, we should emphasize that the principles of two-stage radical treatment for chronic osteomyelitis - where residual bone cavity grafting following necrotic sequestrectomy achieves sustained remission — were previously established in studies by our department and clinic staff . The critical importance of the initial debridement stage is supported by Anikin et al. (2022), who described multi-stage surgical management of chronic gunshot-induced calcaneal osteomyelitis involving sequestrectomy and wound defect reconstruction. Their findings regarding radical surgical debridement and adequate drainage requirements align with our results .
The soft tissue reconstruction strategy in tissue-deficient areas deserves particular attention. Moscow colleagues have successfully employed partially de-epithelialized sural flaps for tibial distal third osteomyelitis treatment, confirming the efficacy of local tissue transfer techniques . Vorotnikov et al. (2022) further demonstrated the clinical effectiveness of locoregional perforator island flaps for soft tissue coverage, which correlates with our reconstructive approach .
The external fixation application for stabilized debrided bone fragments represents another crucial aspect. Ivanov (2009) highlighted the role of external fixation in managing open fractures and chronic osteomyelitis, especially in polytrauma patients . Comparable outcomes were reported in international studies where combined external fixation and soft tissue reconstruction prevented limb amputation in severe extremity injuries .
4. Conclusion
This clinical case demonstrates the efficacy of a combined surgical approach for managing chronic, recurrent osteomyelitis complicated by deep trophic ulcers. The treatment protocol—incorporating radical surgical debridement, external fixation, and local tissue reconstruction —aligns with contemporary management strategies for such complex cases and is supported by existing literature evidence.
Three key findings emerge:
· isolated application of any single surgical modality would inevitably lead to disease recurrence and potential limb loss;
· the staged multidisciplinary approach addresses all pathological components (infection control, bone stabilization, soft tissue coverage).
This algorithm shows particular clinical value for complex cases, featuring:
· significant soft tissue deficiency;
· high recurrence risk;
· multiple previous surgical interventions.
The protocol warrants consideration in clinical practice, especially for complicated presentations where conventional treatments prove inadequate. Its success underscores the importance of combining radical infection control measures, mechanical stabilization and vascularized tissue reconstruction as interdependent therapeutic pillars in refractory osteomyelitis management.