ADENOID CYSTIC CARCINOMA OF THE LACRIMAL GLAND – A CASE REPORT

Валканов С.¹, Валканов П.¹, Славейков К.², Трифонова К.², Попхаритов А.³, Танев И.4, Петров Б.¹
1 Клиника нейрохирургии, 2 офтальмологическая клиника, 3 хирургическая клиника, Университетская больница Стояна Кирковича, Стара-Загора, Болгария, 4 клиника офтальмологии, Университетская больница «Александровска», София, Болгария
АДЕНОИДНАЯ КИСТОЗНАЯ КАРЦИНОМА СЛЕЗНОЙ ЖЕЛЕЗЫ: ИСТОРИЯ БОЛЕЗНИ
Аннотация
Аденоидная кистозная карценома - редкая форма злокачественной опухоли с эпителиальным происхождением. Это наиболее распространенная первичная злокачественная опухоль слезной железы, однако она составляет менее 4% от всех новообразований железы. До сих пор существуют разногласия в вопросе оптимального лечения, в основном, касающиеся хирургического подхода и степени радикального удаления тканей. В представленном случае показано решение вопросов диагностики и лечения аденоидной кистозной карценомы, а также рассмотрены некоторые наиболее распространенные ошибки.
Ключевые слова: аденоидная кистозная карценома, слезная железа, терапевтический подход.
Valkanov St.¹, Valkanov P.¹, Slaveykov K.², Trifonova K.², Popharitov A. ³, Tanev I.4, Petrov B.¹
¹ Neurosurgery clinic, ² Ophthalmology clinic, ³ Surgery clinic, University hospital „Prof. Stoyan Kirkovich, MD”, Stara Zagora, Bulgaria, 4Ophthalmology clinic, University hospital „Aleksandrovska“, Sofia, Bulgaria
ADENOID CYSTIC CARCINOMA OF THE LACRIMAL GLAND – A CASE REPORT
Abstract
Adenoid cystic carcinoma is a rare form of malignant neoplasm with epithelial origin. It is the most common primary malignat neoplasm of the lacrimal gland, yet it is responsible for less than 4% of all neoplasms of the gland. There are still controversies about the optimal treatment, mainly concerning the surgical approach and the degree of radical removal of tissues. The presented case is a good example for the diagnostic and treatment dillemas when dealing with adnoid cystic carcinoma of the lacrimal gland, as well as some of the most common mistakes made.
Keywords: adenoid cystic carcinoma, lacrimal gland, therapeutic approach
Adenoid cystic carcinoma (ACC) of the lacrimal gland a rare form of malignant neoplasm with epithelial origin (1). It is the most common primary malignat neoplasm of the lacrimal gland, yet it is responsible for less than 4% of all neoplasms of the gland (2-4). Most individuals are diagnosed with the disease in the fourth through sixth decade of life (5), and rarely during childhood (6, 7). There are still controversies about the optimal approach for treating the neoplasm. Some author recommend a more conservative approach during surgery, followed by radiation or proton therapy (8). Others support radical evisceration with or without removal of surrounding bone structures as the most appropriate method of treatment (9). In general patients with ACC of the lacrimal gland have poor prognosis, which makes the choice of teurapethic approac difficult (10).
The presented case is a good example for the diagnostic and treatment dillemas when dealing with adnoid cystic carcinoma of the lacrimal gland.
CASE REPORT: We present a case of a 79 y.o female patient, operated on in another hospital in 2010 for a soft tissue formation in the left orbit. No material was taken for histological examination. Four moths after surgery, the patient enters the neurosurgery clinic in University hospital Stara Zagora with complaints of constant pain and swelling in the same area.
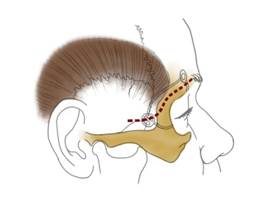
Fig.1 Transsupercilliary superlateroorbitotomy
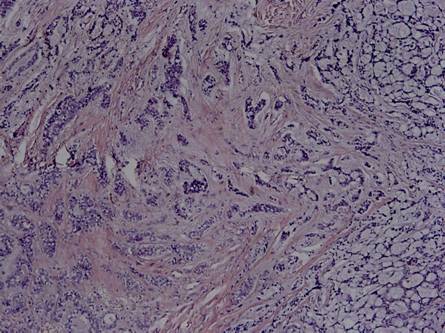
Pic 1. № 2008, 2009 from 28.06.2010г. – adenoid cystic carcinoma
The orbit computer tomography (CT) establishes a soft tissue-equivelent tumor formation in the upper lateral part of the left orbit, extending to lateral orbital structures. Upon admission the patient and no focal neurological symptoms and no visual impairement. A left-sided osteoplastic frontoorbital craniotomy by V. Busarski was preformed (Fig.1), after which the tumor formation was extirpated en block under optic magnification. The formation did not affect the surrounding soft tissues and bone structures. The upper lateral orbital rim waas restored. Histology showed adenoid cystic carcinoma (Pic. 1).

Fig.2 Tumor formation
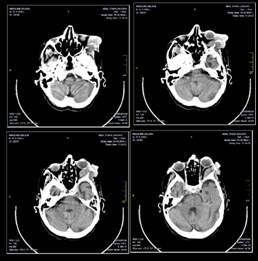
Fig.3 Preoperative CT
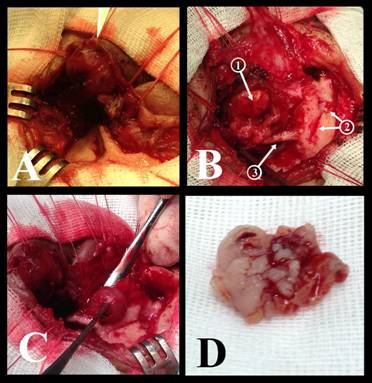
Fig.4 А- Extracranial part of the neoplasm; B 1- bulbus oculi, 2- previous craniotomy, 3 – processus frontalis; C- Dissection of the intra-orbital part of the tumor formation; D – Extirpated intracranial portion of the tumor formation.
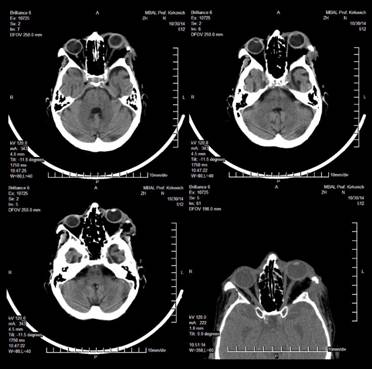
Fig.5 Postoperative CT
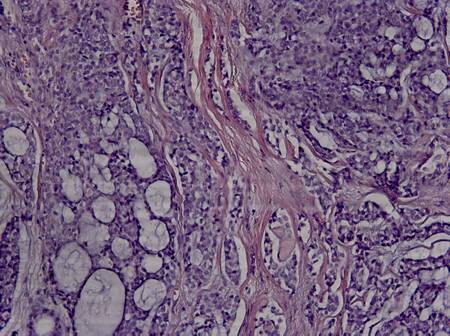
Pic 2. № 1903, 1904 from 30.10.2014г. – recurrence of adenoid cystic carcinoma
Postoperative radio- and chemotherapy was recommended to the patient, which she did not comply with. In September 2014 the patient reenters the clinic with a relapse of the tumor formation. The size of the formation was 2/3 sm, with hard elastic consistency, adherent to underlying structures, slightly painful on palpation with ulcerations of the overlaying skin (Fig. 2). CT of orbits confirms reccurance of a tumor formation on the left periorbitally, covering and lysing the squama of the temporal os, lateral retroorbital space, lateral rectus muscle and processus forntalis of os zygomaticum (Fig. 3). From the ophthalmologic status: Visus of the right eye is 0,7, visus of the left eye is perceptio et proection lucis certa. The right eye is pseudophacic with an intraocular lens. The left eye has a corneal adherence to the iris at 6 o’clock on 3 mm from the limbus. Anteriro chamber is uneven, the pupil is streched torward 6 o’clock and the lens is completely opaque. The patient was taken for reoperation, the extracranial part of the tumor formation was dissected (Fig.4А) and removed untill healthy tissue was reached. Processus frontalis os zygomaticum was lysed to missing (Fig. 4B). The intraorbital part of the tumor formation was disseted and extirpated en block (Fig. 4 C, D) and usures were found on the lateral wall of the orbit (Fig. 5). Histology confirmed recurrance of adenoid cystic carcinoma (Pic. 2).
Adenoid cystic carcinoma is an unusual tumor. Despite its rarety it is the second most common epithelial neoplasm of the lacrimal gland, after benign pleomorphal adenoma and it is the most common malignant neoplasm of the gland (11).
Reoccurance is common until the fourth year after excision. The tumor usually spread via local invasion, and less likely with distant metastasis. In accordance with the dissemination methods in recent years there is a tendency for radical surgery with removal of the neighbouring orbital bones (radical orbitectomy) in combination with radio- and cehmotherapy (2-5; +12-+18). Even with this radical approach some author discuss poor prognosis for patients with the disease (13; 14).
The presented case is an example for the diagnostic and treatment dilemma when facing adenoid cystic carcinoma of the lacrimal gland. In our case the patient had soft lesion in the region of upper lateral orbital rim, wich was treated without the required preoperative diagnostics and preparations. A CT was appropriate, which even then would have shown that the tumor formation had an intraorbital part. The surgical approach would have been different – frontoorbital craniotomy would have provided an easier access to the formation and extripation en block. Another error was the lack of histological verification of the lesion. During the second hospitalisation of the patient, in our hospital, a more appropriate action would have been evisceration. The relatevely early diagnosis of the neoplasm, the macroscopic characteristics (capsulated), the lack of histological verification of the previous incision, as well as the completely preserved functions of the eye were argument for the lack of evisceration. There are some author who prefer a more conservative approach during treatment of ACC of the lacrimal gland (8). The refusal for radio- and chemotherapy from the patient after dehspitalisation also supports the reoccurance.
Adenoid cystic carcinoma is the most common malignat neoplasm of the lacrimal gland. It spreads usually by local invasion and distant metastasis. Surgical removal, followed by radio- and chemotherapy is the only right approach to treatment of the disease. The surgical intervention should be preceded by serious preoperative diagnostics. Appropriate operative access must be chosen, which allows total extripation, and when needed evisceration with removal of the affected bone structures.
References
- Font RL, Smith SL, Bryan RG. Malignant epithelial tumors of the lacrimal gland: a clinicopathologic study of 21 cases. Arch Ophthalmol 1998;116:613–6
- Shields JA Epithelial tumors of the lacrimal gland: primary carcinomas. Shields JAed.Diagnosis and Management of Orbital Tumors. Philadelphia, Pa WB Saunders Co1989;267- 272.
- Shields JABakewell BAugsburger JJFlanagan JC Classification and incidence of space-occupying lesions of the orbit: a survey of 645 biopsies. Arch Ophthalmol. 1984;1021606- 1611.
- Shields CLShields JAEagle RCRathmell JP Clinicopathologic review of 142 cases of lacrimal gland lesions. Ophthalmology. 1989;96431- 435.
- Font RLGamel JW Adenoid cystic carcinoma of the lacrimal gland: a clinicopathologic study of 79 cases. Nicholson DHed.Ocular Pathology Update. New York, NY Masson Publishing USA1980;277- 283.
- Dagher GAnderson RLOssoinig KCBaker JD Adenoid cystic carcinoma of the lacrimal gland in a child. Arch Ophthalmol. 1980;981098- 1100.
- Tellado MVMclean IWSpecht CSVarga J Adenoid cystic carcinomas of the lacrimal gland in childhood and adolescence. Ophthalmology. 1997;1041622- 1625.
- Asikin Natanegara IAA, Koornneef L, Veenhof K, et al. An alternative approach for the management of adenocystic carcinoma of the lacrimal gland. Orbit 1990;9:101–105.
- Marsh JL, Wise DM, Smith M, Schwartz H. Lacrimal gland adenoid cystic carcinoma: intracranial and extracranial en bloc resection. Plast Reconstr Surg 1981;68:577–585.
- Esmaeli B, Ahmadi MA, Youssef A, et al. Outcomes in patients with adenoid cystic carcinoma of the lacrimal gland. Ophthalmic Plast Reconstr Surg 2004;20:22–26.
- Vasantha Thavaraj, M.R. Sridhar, A. SethP and L.S. Arya. Adenoid Cystic Carcinoma of the Lacrimal Gland. Indian Joumal of Pediatdcs, Volume 70---September, 2003, p 751 – 753.
- Font RLGamel JW Epithelial tumors of the lacrimal gland: an analysis of 265 cases. Jakobiec FAed.Ocular and Adnexal Tumors. Birmingham, Ala Aesculapius1978;787- 805.
- Henderson JW Adenoid cystic carcinoma of the lacrimal gland: is there a cure? Trans Am Ophthalmol Soc. 1987;85312- 334.
- Jakobiec FA Discussion of Henderson JW. Adenoid cystic carcinoma of the lacrimal gland: is there a cure? Trans Am Ophthalmol Soc. 1987;85314- 337.
- Lee DACampbell RJWaller RRIlstrup DM A clinicopathologic study of primary adenoid cystic carcinoma of the lacrimal gland. 1985;9212- 34.
- Byers RMBerkeley RGLuna MHesse R Combined therapeutic approach to malignant lacrimal gland tumors. Am J Ophthalmol. 1975;7953- 55.
- Wright JEStewart WBKrohel GB Clinical presentation and management of lacrimal gland tumours. Br J Ophthalmol. 1979;63600- 606.
- Gamel JWFont RL Adenoid cystic carcinoma of the lacrimal gland: the clinical significance of a basaloid histologic pattern. Hum Pathol. 1982;13219- 225.