NEW TACTIC FOR THE TREATMENT OF CHOLEDOCHOLITHIASIS
NEW TACTIC FOR THE TREATMENT OF CHOLEDOCHOLITHIASIS
Abstract
Introduction. Along with the active development of endoscopic transpapillary interventions, the causes that complicate and make ineffective the usage of endoscopic operations, as the "gold standard" for the treatment of choledocholithiasis, are being studied simultaneously. Similar conditions in modern literature are united by the term "difficult" choledocholithiasis.
The purpose of the study is to prove the effectiveness of the usage of our algorithm in the treatment of the patients with" difficult" choledocholithiasis.
Material and methods. The results of treatment of 295 patients with "difficult" choledocholithiasis were analyzed. The main group consisted of 177 patients who were treated with using of the treatment algorithm suggested by us.
Results. Choledocholithotomy was done for the 67 patients (56.78%) of the control group with endoscopic unresolved choledocholithiasis. In 32 patients (27.12%) of the control group and in 7 patients (5.35%) of the main group, endobiliary stenting was used as the final method of treatment. In the group where our algorithm was used the open operation was performed in 7 cases (3.95%). The mortality rate in the main group is significantly lower than in the control group: 1.13% vs. 4.24%.
Conclusion. The usage of the algorithm developed by us proves the effectiveness of the endobiliary stenting in the treatment of "difficult" choledocholithiasis (90.7% of positive results).
1. Introduction
According to various authors, gallstone disease complicated by choledocholithiasis occurs from 12.7 to 29.4 % of cases , and it is often the cause of such serious complications as mechanical jaundice, cholangitis, liver abscesses, septic shock, acute pancreatitis, stenosis of the large duodenal papilla, liver failure and biliary cirrhosis , , .
With the development of endoscopic technologies, minimally invasive treatment of cholelithiasis has become the "gold standard" and the usage of the transpapillary and laparoscopic technologies is widely implemented in specialized centers.
Currently, if the appropriate medical equipment is available, treatment of choledocholithiasis in patients with concomitant cholecystolithiasis is carried out in two stages , , . The first step is a transpapillary removal of stones from the common bile duct, the next one is a laparoscopic cholecystectomy , , .
Many authors attribute the ineffectiveness of modern x-ray endoscopic techniques, even with their systematic and algorithmic usage, to the peculiarities of the ductal system, the size and location of stones and the anatomy of the bilioduodenal region, which form the concept of "difficult" choledocholithiasis , , .
The accumulated clinical experience and the data of the analysis of treatment allowed us to develop a curing algorithm for patients with a difficult choledocholithiasis.
2. Research methods and principles
In our study, we provided a retrospective analysis of the results of treatment of 295 patients who were treated from 2000 to 2019 at the Center of Liver and Pancreas Surgery on the basis of the Belgorod regional clinical hospital of St. Joasaph with diagnosed "difficult" choledocholithiasis. The main group consisted of 177 patients treated from 2008 to 2019, on whom the proposed treatment algorithm was used. The control group included 118 patients with "difficult" choledocholithiasis who were treated from 2000 to 2007. The patients were divided by gender and age in the following way (Table 1).
Table 1 - Gender and age of patients of the main and control groups
Total number of patients | Control group (2000 – 2007) | Main group (2008 – 2019) | ||
118 | 177 | |||
Women | abs. | 72 | 111 | |
rel. | 61.02 | 62.71 | ||
Men | abs. | 46 | 66 | |
rel. | 38.98 | 37.29 | ||
Average age of women | 66.34 | 66.81 | ||
Average age of men | 64.36 | 65.95 | ||
Maximum age | 89 | 92 | ||
Minimum age | 32 | 36 | ||
The number of patients at the age of 60 and older | abs. | 94 | 126 | |
rel. | 72.87 | 71.19 | ||
There were 111 women (62.71%) and 66 men (37.29%) out of the total number of patients of the main group. The average age of the patients was 66.5 (66.81 for women and 65.95 for men). The maximum age of patients was 92 and the minimum age was 32. The number of patients at the age of 60 and older was 126 (71.19%).
According to our proposed algorithm of treatment, depending on the clinical picture and further surgical tactics, all patients of the main group with "difficult choledocholithiasis" were divided into 4 groups:
1) the patients who had a predominant clinic of mechanical jaundice and cholangitis (septic shock) (n — 111; 62.71%);
2) the patients with pain-free (asymptomatic) choledocholithiasis, confirmed by sonography investigation (biliary hypertension, choledocholithiasis) (n — 24; 13.55%);
3) the patients with acute biliary pancreatitis (n — 27; 15.25%);
4) the patients with residual choledocholithiasis and an external bile fistula on the drainage (n-15; 8.47%).
The results were based on the data of the mortality rate in the main group, in which the algorithm developed by us was used, and in the control group.
All patients underwent an integrated testing, which includedthe clinical and anamnestic examination (the presence of pain and its relationship with the appearance of the skin and sclera jaundice, the darkening of urine, the appearance of aholic faeces, the temperature reaction and its type), clinical and laboratory examination, ultrasound investigation of the abdominal cavity organs, fistulography in patients with residual choledocholithiasis.
General clinical laboratory examinations included full blood panel, urine analysis, blood chemistry, determination of body temperature, electrocardiography, chest fluorography, blood coagulation and the acid-base state of the blood.
All patients underwent endoscopic transpapillary interventions with endoscopic retrograde cholangiopancreatography (ERCP). We also evaluate the diameters of the common bile duct, lobular ducts of the liver, the size of the stones, the length and diameter of the intrapancreatic part of the common bile duct. These criteria determining whether the stones can be independently removed from the common bile duct (CBD) or extracted by the Dormia’s basket usage, in order to avoid infringing of the last.
3. Main results
The results of treatment of the control group patients. All patients of the control group started treatment with using endoscopic interventions, for 7 of which (5.93%) an adequate transpapillary interventions were not done (5 patients after gastric resection for B-II with a long adductor loop, 2 patients with a "large" parapapillary diverticulum).
In 56.78% of cases (n – 67) of endoscopic unresolved choledocholithiasis surgical choledocholithotomy with a primary suture of the common bile duct or choledocholithotomy in combination with choledochoduodenoanastomosis, hepaticoejunoanastomosis, external drainage of the common bile duct or transduodenal papillosphincteroplasty were performed. The complications developed in 19 (28.5%) patients (bleeding, bile leakage, cholangitis, sepsis, multiple organ failure). 5 patients died among them.
In all cases, the cause of death after surgical interventions with restored bile flow was the development of multiple organ failure at the background of cholangiogenic sepsis.
32 patients (27.12%) with endoscopic unextractable extrahepatic bile duct stones out of the 118 patients of the control group, ERCP with endobiliary stenting were the final method of treatment. It was connected with a high operational and anesthetic risk and the denial of radical surgical treatment.
The remaining 16 patients were able to perform endoscopic lithoextraction after a course of oral litholytic drug therapy (lasting at least 6 months) and a common bile duct stenting.
The overall mortality rate of the control group was 4.24%.
Results of treatment of the main group of patients. Multiple choledocholithiasis was diagnosed in 48.57% of cases. The average size of the common bile duct stones was 11.66±3.01 mm. The maximum size of stones was 22 mm and the minimum size was 7 mm.
For the patients with cholangitis drainage operations (nasobiliary drainage, stenting of the common bile duct) with a sanitation purpose were performed. Between the endoscopic sessions, conservative measures aimed at the resolution of jaundice and cholangitis, prevention and treatment of complications were carried out. After stopping the phenomena of cholangitis, if the stone cannot be resolved, stenting of the common bile duct was performed.
In patients with acute biliary pancreatitis, endobiliary stenting was performed until the complete relief of the phenomena of pancreatic edema (ultrasound control, amylasemia) and mechanical jaundice.
In the case of residual choledocholithiasis with the presence of an external bile fistula, papillosphincterotomy was added with stenting of the common bile duct to eliminate the bile fistula, followed by an attempt of endoscopic lithoextraction.
For all patients with diagnosed "difficult" forms of choledocholithiasis endobiliary stenting was performed for a period of at least 6 months. According to the ultrasound investigation and ERCP data, long-term stenting in combination with the usage of the litholytic drug therapy (medication of chenodeoxycholic- and ursodeoxycholic acid) decrease the size and density of the common bile duct stones. After 6 months, it allowed to perform the endoscopic lithoextraction in 62 cases (35.03%). Thus, according to the ERC data, the size of stones decreased from 11.66±3.01 mm to 10.82±2.82 mm.
In other cases of unresolved choledocholithiasis, all patients underwent multislice computed tomography of the abdominal organs to determine the density of the CBD stones, in order to predict the effectiveness of subsequent remote stroke-wave lithotripsy. Thus, a positive result was achieved in 97 patients, which accounted for 54.5% of cases of "difficult" choledocholithiasis.
In 7 cases (3.95%) of the ineffectiveness of the treatment and diagnostic measures, open surgery was performed (choledocholithotomy with or without bile duct drainage, biliodigestive anastomosis, transduodenal papillosphyncteroplasty). At the same time, there were 2 cases of fatal outcome in this group. The cause of death was multi-organ failure at the background of the septic shock. The overall mortality rate of the main group was 1.13%.
4. Discussion
Open laparotomic operations in the treatment of choledocholithiasis, as well as the bilioduodenal drainage nowadays are performed in the extreme cases, and they are the operations of reserve (despair) when all minimally invasive methods of treatment of choledocholithiasis and correction of bile flow are exhausted , .
For 10 out of 177 patients of the main group endoscopical unextractable CBD stones, ERCP with sphincterotomy, bilioduodenal stenting was the final method of treatment. It was connected with a high operational and anesthetic risk. The minimum age of patients of this group was 76 and the average age was 81.57 , , , .
The scheme of the treatment algorithm in "difficult" choledocholithiasis developed by us is shown in Figure 1.
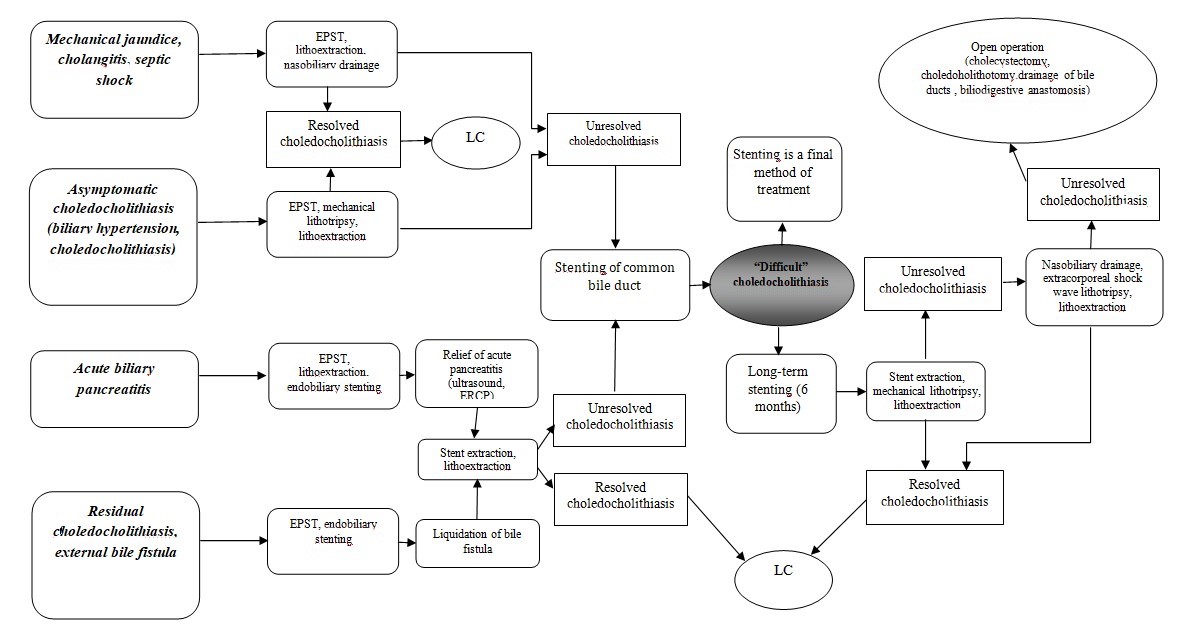
Figure 1 - Treatment Algorithm for patients with "difficult" choledocholithiasis
5. Conclusion
Our experience has shown that the complex usage of described this algorithm are effective in most cases and allows almost completely to refuse “open” operations from laparotomic access (cholecystectomy, choledocholithotomy, bile duct drainage, biliodigestive anastomosis). “Open” operations were done in 3.95 % of cases.
Endobiliary stenting as a final method of treatment has taken place in 5.65%. It was connected with a high operational and anesthetic risk. The mortality rate in the main group was significantly lower than in the control group, which ranges 1.13% vs. 4.24% of cases.
In conclusion, it can be noted that in the surgical treatment of patients with endoscopically unresolved ("difficult") choledocholithiasis and high operational and anesthetic risk the treatment algorithm, which include the active usage of a long-term endobiilary stenting, can be recommended.