STUDYING THE FORMATION OF E-HEALTH ON THE BASIS OF INDUSTRY 4.0: APPLYING THE EXPERIENCE FOR RUSSIAN E-HEALTH. IS THERE AN OPPORTUNITY WINDOW FOR THE INNOVATION-GUIDED PROCESS INTEGRATION OF E-HEALTH IN RUSSIA?

ИЗУЧЕНИЕ ФОРМИРОВАНИЯ ЭЛЕКТРОННОЙ СИСТЕМЫ ЗДРАВООХРАНЕНИЯ НА БАЗЕ ИНДУСТРИИ 4.0: ПРИМЕНЕНИЕ ИМЕЮЩЕГОСЯ ОПЫТА В РОССИЙСКОМ ЭЛЕКТРОННОМ ЗДРАВООХРАНЕНИИ. ВОЗМОЖНА ЛИ ИННОВАЦИОННАЯ ИНТЕГРАЦИЯ ЭЛЕКТРОННОЙ СИСТЕМЫ ЗДРАВООХРАНЕНИЯ В РОССИИ?
Обзорная статья
Бутнева А.Ю.1, Гумерова Г.И.2, Шаймиева Е.Ш.3, *
1 ORCID: 0000-0002-4892-912;
2 ORCID: 0000-0002-5198-7576;
3 ORCID: 0000-0002-9588-0199;
1 Мангеймский университет, Германия;
2 Финансовый университет при Правительстве Российской Федерации, Москва, Россия;
3 Казанский инновационный университет имени В. Г. Тимирясова, Казань, Россия
АннотацияВ данной статье представлен обзор работ зарубежных (с российской точки зрения) авторов в области электронной системы здравоохранения Индустрии 4.0. Затем анализируется научный вклад в этой области на протяжении трёх периодов (основных этапов), влияющих на формирование электронной системы здравоохранения: внедрение дистанционной медицины по всему миру, социально-технические параметры процесса внедрения (оптимизация технологий дистанционной медицины) и внедрение электронной системы здравоохранения в условиях современной России. В данном исследовании рассматривается возможность инновационного внедрения электронной системы здравоохранения на основе европейского опыта Индустрии 4.0 для получения конкретных инструментов внедрения электронной системы здравоохранения в России. По результатам проведённого исследования авторы выделили семь аспектов, способствующих инновационному внедрению в России электронной системы здравоохранения: определение понятия электронной системы здравоохранения; переосмысление «третьего пути» в контексте развития электронной системы здравоохранения; понимание как социальной, так и технической частей социально-технического подхода к российской электронной системе здравоохранения; уточнение взаимоотношений между основными субъектами коммерческой модели электронной системы здравоохранения; определение положения «дистанционной медсестры»; уточнение различий между системами взаимодействия, ориентированными на цену и на количество, горизонтальным и вертикальным процессом внедрения. Результаты обзора способствуют общему пониманию технологий дистанционной медицины и проливают свет на направления формирования российской электронной системы здравоохранения.
Ключевые слова: электронная система здравоохранения, Индустрия 4.0, дистанционная медицина, социально-технические параметры, процесс внедрения.
STUDYING THE FORMATION OF E-HEALTH ON THE BASIS OF INDUSTRY 4.0: APPLYING THE EXPERIENCE FOR RUSSIAN E-HEALTH. IS THERE AN OPPORTUNITY WINDOW FOR THE INNOVATION-GUIDED PROCESS INTEGRATION OF E-HEALTH IN RUSSIA?
Review article
Butneva A. Yu.1, Gumerova G.I.2, Shaimieva E.Sh.3, *
1 ORCID: 0000-0002-4892-912;
2 ORCID: 0000-0002-5198-7576;
3 ORCID: 0000-0002-9588-0199;
1 University of Mannheim, Germany;
2 Financial University under the Government of the Russian Federation, Moscow, Russia;
3 Kazan Innovative University named after V. G. Timiryasov (IEML)" Kazan, Russia
AbstractThis paper reviews the works of foreign (from the Russian perspective) authors in the field of e-health Industry 4.0. The scientific contribution in this area is then analyzed during three periods or fundamental stages that affect the formation of e-health: worldwide introduction of telemedicine, socio-technical parameters of process integration (optimization of telemedical technology), and integration of e-health in modern Russia. The study examines the possibility of innovative integration of Russian e-health based on European experience from Industry 4.0, aiming to derive specific tools for the integration of e-health in Russia. As a result of the study, the authors identified seven aspects that contribute to the innovative integration of Russian e-health: definition of e-health, re-definition of the “third path” in the context of e-health development; understanding of both social and technical parts of the socio-technical approach to Russian e-health; refinement of the relationship between the main actors in the e-health business-model; determination of the "teleschwester" [telesister] position; elaboration of the differences between price-and quantity-oriented operational systems, horizontal and vertical process integration. The results of the review contribute to the overall understanding of telemedicine technologies and shed light on directions in the formation of Russian e-health.
Keywords: e-health, Industry 4.0, telemedicine, socio-technical parameters, process integration.
The World Health Organization (WTO) defines e-health or digital health as “the use of information and communication technologies (ICT) for health.” [18] Thereby, e-health can be implemented at the global, national, and regional levels, serving the purpose of improving healthcare standards worldwide. However, the degree of integration of e-health into distinct healthcare systems varies significantly across WTO members, with only 58% of member states having an e-health strategy and Russia absent in this list [18]. Thus, effectively embedding e-health structures, specifically, into the Russian healthcare branch results in a considerable challenge for scholars and policymakers, which gives relevance to this study.
Since 2017, Russian healthcare has been engaged in providing services in electronic format, i.e., telemedicine services, developing a region-specific business model for e-healthcare [11], [12], [13]. Albeit different approaches were introduced to implement e-health in Russia, existing studies are still lacking a general comprehension of previous e-health experience and a detailed analysis. Hereby we attempt to narrow this gap by considering the experience of Industry 4.0, which started in 2011 in Western Europe, in order to optimize the process of developing Russian e-health care [14], [15], [16]. Introduction and refinement of the fundamental concepts and solutions proposed by Industry 4.0 might then resolve many organizational and management issues emerging during the implementation of e-health in Russia in the prevention mode [15], [16].
Theoretical Approaches to E-Health
Häcker et al. examine the core issues related to development and application of telemedicine and e-health from the strategic perspective, which evaluates the healthcare industry as a single commercial entity by considering the stock market multipliers [5]. The authors also refer to their vision of an e-health-business-model, which includes process integration of information systems [5]. This study represents a scientific interest for researchers in the aspect of telemedicine entering the share market (IPO) [5]. Häcker et al. denote the competitive advantage of firms in the price-to-quality ratio that provide online medical service, mainly in the area of cardiovascular diseases and diabetes [5]. According to the authors, novel models of merger and acquisition, as well as the optimal use of venture capital, are preliminarily tested on highly developed telemedicine markets in Finland, USA, and Israel and then, subsequently, adopted by German firms [5].
Gersch M., Liesenfeld J. set up the baseline model of e-health and focus on the main types of economic activity for the use in Ambient Assisted Living (AAL) model while studying existing internet-platforms [6]. T. Mathar, on the contrary, concentrates on digital patients as a target group for medical e-service rather than on general model framework of internet-based healthcare [10]. Mathar’s study emphasizes the following aspects concerning digital patients: information and communication technologies in the S&T system of healthcare; theoretical and practical directions of social determinism; micro-politics of the healthcare system; “third path” – interactive approach in research and development; technical issues in everyday life of patients; logic and boundaries of baseline e-health model; model of medical trajectory[10].
In his chapter “Theoretical and practical directions of social determinism”, information and communication technologies are presented as a social construction, where e-medical card and telemonitoring technology represent typical elements of S&T system of healthcare. T. Mathar further explores the work specifics of the so-called “Teleschwester” (telemedical nurse) in the chapter devoted to micro-politics [10]. Thus, a teleschwester [telesister]executes various tasks in telemedical centers: she communicates with doctors and patients, makes preliminary diagnoses, records phases of progress and regress in the healing process of patients and manages the accounting department of hospitals.
Consequently, Mathar refers to telemedical centers as socio-technical networks where interactions between people and digital innovations (so ontologically distinct elements) mainly take place [10]. Hence, the micropolitics of S&T healthcare system denotes various ways of integration of teleschwester in the networks as well as diverse relationship patterns resulting from this innovation.
The discussion above sums up to an e-health-business-model, formulated by T. Lux based on Industry 4.0 [8], [9]. His business-model incorporates the following actors: recipients of medical services (patients who receive medical services in both traditional and electronic ways are considered “digital”); suppliers of medical services, e.g., doctors, consultants, diagnosticians, laboratory assistants; payment agents, i.e., health insurance.
Therefore, nine distinct relationship patterns exist within the e-health system, according to T. Lux: patient-to-doctor (P2D) and doctor-to-patient (D2P); patient-to-insurance (P2I) and insurance-to-patient (I2P); insurance-to-doctor (I2D) and doctor-to-insurance (D2I) [8], [9]. Further, inter-group relations as P2P, D2D, and I2I are also possible in this model framework. To put it in a nutshell, process integration of information systems enables interactions in nine different directions, so its optimization is the main goal of this case [8], [9].
We trace this process of digitalization of healthcare in Germany from the 1960-s to the recent developments emphasizing telemedicine and socio-technical parameters of systems to enhance the general comprehension of e-health and apply specified concepts to Russian healthcare.
The Period of the First. Development of E-Heath from 1960-s to the present: Telemedicine as Intermediate Stage
Telemedicine was invented in Canada, where 1959 first coaxial cable was introduced to the international medical community as a means to exchange x-rays between two hospitals in Montreal. Subsequently, this practice gave birth to an innovative scientific branch – teleradiology, which commemorated the first step towards the digitalization of healthcare in an international context [1], [7].
In the 70-s, the use of ICT-s was extended to various areas of medical practice and a new common expression – telemedicine – has entered the scientific community. From Western literature of that time, we know that telemedicine encompassed telepathology, -dermatology, -surgery and cardiology. This trend indicates that ICTs were gradually integrated into the day-to-day practice of hospitals.
In the 90-s, the informatization of society speeds up, and telemedicine is now replaced by telematics. Telematics combines two strands of new-born science – telecommunication and informatics. Telematic systems enable information transfer between all actors of the healthcare industry, for instance, through the internet or landline. Thus, telematics systems enhance the centralization of telemedical branches and effectively manage communication channels and data storage. Thereby they link administrative tasks of hospital management with healing practices in medical facilities. Under this assumption, telematics is superior to telemedicine [1].
At the beginning of the 21-st century, resulting from modernization of global economic chains, a cumulative term “e-heath” entered the hospitals. E-health translates core concepts of e-commerce to the healthcare specifics, e.g., market of e-medical services. These services include online-provision of drugs, electronic cards for patients, online-consulting and electronic receipts, as well as the possibility of ambulatory, stationary, or telemedical care dependent on the diagnosis.
The Period of the Second. Process Integration of E-Health: A Socio-Technical Approach
Integration of the I&C (information & communication) systems into the dynamic healthcare sector seems very challenging due to its complexity. Given the difficulty of this task, a successful integration of I&C systems requires a preliminary integration of professional processes concerning the hierarchic structure of healthcare. Scientific projects developed in the Industry 4.0 have already shown a significant innovation potential, but they only partially satisfy customer demands. In order to reduce this gap between demand (patients) and supply (providers of I&C systems in charge of technological advancement in hospitals), we need to apply a socio-technical approach for solving the case. This approach directly incorporates the demands of all actors when creating and developing the I&C systems.
According to T. Lux, an individual should have a central position in the created system - social premise [10], [11]. In the healthcare system, a “person” denotes either doctors, patients, medical staff, or hospital administration. Therefore, an e-health-business-model preserves social factor by keeping face-to-face services in emergent hospitalization. Book-keeping, intensive care personal, and staff employed in the palliative area will as well continue doing their work on the spot (see Figure 1).
Lux further notes that technical equipment in hospitals should facilitate and further improve the performance of the actors’ duties in line with the functional requirements - technical premise [8], [9]. Thus, the reform providers face the following challenges on this stage: an appropriate conceptualization and classification of integration networks; maintaining high professionalism in the implementation of medical procedures; a realistic evaluation of innovation and integration potential in different areas of healthcare branch.
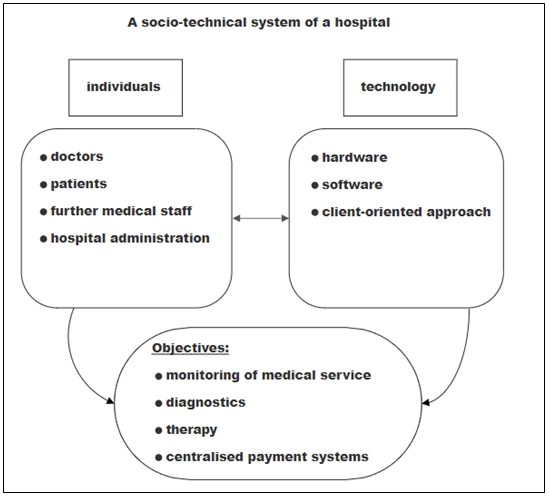
Fig.1 – A socio-technical system of a hospital
Successful process integration within one medical facility and between different facilities requires simultaneous horizontal and vertical integration of different application areas within the healthcare system. Thus, these areas should be structured and distributed, according to the appropriate level, and via IT-supported process monitoring.
All systems that are actively practiced in the medical branch and thus involved in the value-creation process are subject to quantity-oriented payment structures. The value-creation process is thus supported by such information systems that manage documentation, communication and decision-making in the hospitals and are diffused at the operational level, according to their functionality. Operation-based systems of bookkeeping and accounting are subordinate to price-oriented payment structures. Subsequently, a price-oriented payment system is subject both to the controlling department and further superior accounting and monitoring systems (or statistical systems). In case of implementation of ERP systems for IT-support of decision-making concerning managerial issues, an additional adaptation at higher levels of information pyramid is required. Further specification is offered below.
Thus, to derive realistic recommendations for the step-by-step integration of e-health in Russia, the knowledge of the pyramidal classification of information systems in hospitals is required. This classification depicts a fundamental way of structuring the multifaceted construct of a digital hospital subdivided into various layers. Following the logic of this baseline model, we differentiate between administration & regulation and planning & controlling systems based on the extent to which information is concentrated among the actors engaged in the value-generating process at various levels [1], [7].
Hence, taking the example of quantity-oriented operational systems, we can infer from the model that they exhibit a low degree of concentration of information and thus are grouped at the lowest level in the classification. An in-depth understanding of the baseline model presented in Figure 2 will enhance the comprehension of Russian implementation of e-health addressed in this review, since it follows the same triangle shape [15], [16].
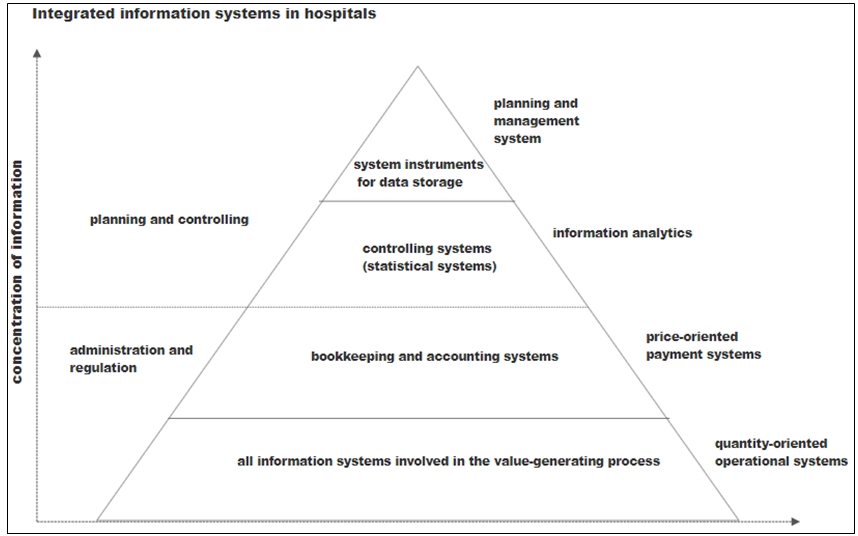
Fig. 2 – Integrated information system in hospitals
The Third Stage: Integration of E-Health in Russia
Since Russian hospitals embody complex constructs of different information systems, we identify several systems, which can be used by medical staff in order to enhance the decision-making process in Russian e-health. Al already mentioned in the theoretical part of the study, the bottom-up contraction of information starts from the transition from quantity-oriented information systems to price-oriented payment systems and continues to the top of the pyramid. Matching of information systems that participate in the value-generating process is mostly based on quantity-oriented operational systems. This satisfies the requirements of medical information systems as well as all technical, organization, and administration systems, which directly support the value-generating process in Russian e-health business model [15], [16].
Given these defining system features, we estimate functional capabilities of state information systems (SIS) in Russia, according to the “Requirements for the state-based medical information systems in states of Russian Federation” in twenty subfields:
- Introduction of legal background material (e-based) concerning a particular state;
- Electronic registry;
- The organization of emergency assistance, including air ambulance and aeromedical evacuation services;
- Provision of medical service with telemedical assistance;
- Consideration of regional demographic features as well as the resource capabilities of local healthcare systems;
- Implementation of specific categorized patient registers;
- Stable supply of medical drugs and other industry-specific goods, including concessional goods;
- Integration of e-medical patient cards within states of the Russian Federation;
- Support of the decision-making concerning healthcare management at all organizational levels;
- Introduction of state health standards, adjusted for regional specifics;
- Functional integration of blood transfusion service;
- Provision of sanitary-epidemiological monitoring;
- Consideration of preventive check-ups in the population;
- Functional integration of immune prophylactics;
- Regional laboratory information systems;
- Region-based centralized archives for storage of medical imaging;
- Automatization of medical service for different categories of citizens (diversification);
- Monitoring of delivery care;
- Introduction of strict document verification systems, e.g., disability certificate, preferential prescription pads;
- An integrated medical data bus.
SIS-s of states of the Russian Federation can contain other sub-systems, which are not included in the primary and extended list of functional capabilities. Such sub-systems are presented as follows:
- E-library of supporting decision-making systems for the doctors; Regional or local online-portals for healthcare-related matters;
- Private online accounts of patients;
- Anonymized medical information for science & research;
- Online-portals for the medical community.
Finally, we derive several baseline indicators from Industry 4.0 and Russian law, which are supposed to be changed within the five years. These measures include the number of patients-users of the online-portal “My health”, the fraction of medical organizations using online-portals as well as the percentage of medical organizations, which grant access of online medical care to their patients, for instance, via “My health” [11], [17].
Research results
This study reviewed the works of foreign (from the Russian perspective) authors in the field of e-health Industry 4.0. The scientific contribution in this area was analyzed during three periods or fundamental stages that affect the formation of e-health: worldwide introduction of telemedicine, socio-technical parameters of process integration (optimization of telemedical technology), and integration of e-health in modern Russia. Our theoretical analysis of the formation of e-health in Germany yielded following findings, which might enhance the development of Russian e-health and enrich the existing knowledge in this field:
- The meaning and substance of “third path” or “third way” in context of e-health development were analyzed in comparative perspective. Consequently, “third path” was defined as a philosophical concept of balance between human beings and technological design, neither subjective nor objective, where people and innovations made by people should modestly co-exist and complement each other. E-health was then defined as “the use of information and communication technologies (ICT) for health.”
- The comprehension of both social and technical parts of e-heath was proven pivotal for the implementation of Russian e-health. According to discussed empirical works in this field, an individual is expected to have a central position in the created system – a social premise. Therefore, a Russian e-health-business-model can preserve social factor by keeping face-to-face services in emergent hospitalization. Book-keeping, intensive care personal, and staff employed in the palliative area will as well continue doing their work on the spot. Technical equipment in Russian hospitals will then facilitate and further improve the performance of the actors’ duties in line with the functional requirements – a technical premise.
- The main actors of e-health-business-model were defined within the interaction system of e-health, consisting of recipients of medical services, suppliers of medical services, and payment agents, i.e., health insurance provided by the state or private insurance companies – and their mutual dependence in nine possible forms (P2D, D2P, P2I, I2P, I2D, D2I, P2P, D2D, I2I) based on standardized medical information systems.
- The functions of “teleschwester" [telesister] in Russian healthcare were derived as following: interpersonal communication, preliminary diagnostics, records of progress and regress in the healing process of patients, management of the accounting department of hospitals.
- Differences between price- and quantity-oriented operational systems in Russian healthcare were scrutinized so that all systems that are involved in the value-creation process in the e-health business model were considered subject to quantity-oriented payment structures.
- Differences between horizontal and vertical integration were proven sufficient for designing Russian e-health business model. Hereby horizontal integration denotes the integration along the value-creation-chain of products and vertical integration implies merging many hierarchic levels via integration of technical innovations.
- Various types of support through e-health were proposed for Russian e-health: monitoring of medical service, diagnostics, therapy, centralization and coordination of payment structures; administration & regulation and planning & controlling systems based on the extent to which information is concentrated among the actors engaged in the value-generating process at distinct levels. Functional capabilities of state information systems (SIS) in Russia were estimated, according to the “Requirements for the state-based medical information systems in states of Russian Federation” in twenty subfields.
However, the indicators presented in this review article need further theoretical examination and thorough empirical consideration. Hence, a supplementary operationalization of suggested concepts in Russian e-health undoubtedly constitutes a promising prospect for future research in this area.
| Конфликт интересов Не указан. | Conflict of Interest None declared. |
Список литературы / References
- Bauer, C. E-Health: Datenschutz und Datensicherheit / Bauer, C., F. Eickmeier & M. Eckard.// Wiesbaden: Springer Fachmedien GmbH. – 2018
- Приказ Министерства здравоохранения РФ от 30 ноября 2017 г. № 965н “Об утверждении порядка организации и оказания медицинской помощи с применением телемедицинских технологий”. [Электронный ресурс] – URL: http://www.garant.ru/products/ipo/prime/doc/71751294/ (дата обращения: 10.06.2020).
- EU e-Health policy, European Commission. (n.d.) [Electronic resource] – URL: http://ec.europa.eu/health/ehealth/policy/index_en.htm (accessed: 10.06.2020).
- Fragen und Antworten zur elektronischen Gesundheitskarte und zum E-Health-Gesetz [Questions and answers tot he electronic healthcare card and e-health law]. [Electronic resource] – URL: https://www.bundesgesundheitsministerium.de/service/begriffe-von-a-z/e/e-healthgesetz/faq-e-health-gesetz.html. (accessed: 10.06.2020)
- Häcker, J. Markt, Strategien, Unternehmensbewertung / Häcker, J., B. Reichwein & N. Turad // München: Oldenburger Wissenschaftsverlag GmbH. – 2008
- Gersch, M. AAL- und E-Health-Geschäftsmodelle / Gersch, M. & J. Liesenfeld.. Wiesbaden: Springer Gabler. - 2012
- Kunze, H. / Kunze, H. & S. Mutze Oldenbourg: Wissenschaftsverlag GmbH.
- Lucks, K. Praxishandbuch Industrie 4.0. / Lucks, K. // Stuttgart: Schäffer-Poeschel Verlag. - 2017
- Lux, T. E-Health – Begriff und Abgrenzung. In S. Müller-Mielitz & T. Lux (Eds.), E-Health Ökonomie (pp. 39-57). Wiesbaden: Springer Gabler.- 2017
- Mathar, T. Der digitale Patient / Mathar, T. Bielefeld: Transcript Verlag. – 2010
- Министерство здравоохранения РФ [Электронный ресурс] – URL: https://www.rosminzdrav.ru/ministry/61/22/informatsionnye-materialy-po-napravleniyu strategicheskogo-razvitiya-rossiyskoy-federatsii-zdravoohranenie/elektronnoe-zdravoohranenie (дата обращения: 10.06.2020).
- Программа «Цифровая экономика Российской Федерации». [Электронный ресурс] – URL: http://static.government.ru/media/files/9gFM4FHj4PsB79I5v7yLVuPgu4bvR7M0.pdf 9gFM4FHj4PsB79I5v7yLVuPgu4bvR7M0.pdf (дата обращения: 14.03.2020).
- Постановление правительства Рф 447 [Электронный ресурс] – URL: https://telemedicina.ru/news/law/pravila-deyatelnosti-medicinskih-organizacij-v-sfere-cifrovogo zdravoohraneniya, (дата обращения: 10.06.2020).
- Приказ №268 о введение в действие отраслевого классификатора Сложение и комплексные медицинские услуги [Электронный ресурс] – URL: http://www.zakonprost.ru/content/base/25908 (дата обращения: 10.06.2020).
- Приказ № 965 об утверждении порядка организации медицинской помощи с применением телемедицинских услуг. Утвержден приказом Министерства здравоохранения РФ.. [Электронный ресурс] – URL: https://telemedicina.ru/news/law/funktsionalnyie-vozmojnosti-gosudarstvennyih-informatsionnyih sistem-v-sfere-zdravoohraneniya-subyektov-rossiyskoy-federatsii (дата обращения: 10.06.2020).
- Владимирский А. В. Телемедицина: Curatio Sine Tempora et Distantia. / А. В. Владимирский // Москва: Aegitas. – 2016.
- World Health Organization [Electronic resource] – URL: https://www.who.int/ehealth/en/ (accessed: 12.08.2020).
Список литературы на английском языке / References in English
- Bauer, C. E-Health: Datenschutz und Datensicherheit / Bauer, C., F. Eickmeier & M. Eckard. // Wiesbaden: Springer Fachmedien GmbH. – 2018
- Prikaz Ministerstva zdravoohranenija RF ot 30 nojabrja 2017 g. № 965n “Ob utverzhdenii porjadka organizacii i okazanija medicinskoj pomoshhi s primeneniem telemedicinskih tehnologij” [Decree #965 “On the Introduction of the Procedure of Organization of Medical Facilities with the Employment of Telemedical Services]. [Electronic resource] – URL: http://www.garant.ru/products/ipo/prime/doc/71751294/ (accessed: 10.06.2020). [in Russian]
- EU e-Health policy, European Commission. (n.d.) [Electronic resource] – URL: http://ec.europa.eu/health/ehealth/policy/index_en.htm (accessed: 10.06.2020).
- Fragen und Antworten zur elektronischen Gesundheitskarte und zum E-Health-Gesetz [Questions and answers tot he electronic healthcare card and e-health law]. [Electronic resource] – URL: https://www.bundesgesundheitsministerium.de/service/begriffe-von-a-z/e/e-healthgesetz/faq-e-health-gesetz.html. (accessed: 10.06.2020) [in German]
- Häcker, J. Markt, Strategien, Unternehmensbewertung / Häcker, J., B. Reichwein & N. Turad // München: Oldenburger Wissenschaftsverlag GmbH. – 2008 [in German]
- Gersch, M. AAL- und E-Health-Geschäftsmodelle. Wiesbaden: Springer Gabler/ Gersch, M. & J. Liesenfeld.. - 2012[in German]
- Kunze, H. Telemedizin / Kunze, H. & S. Mutze. Oldenbourg: Wissenschaftsverlag GmbH. [in German]
- Lucks, K. Praxishandbuch Industrie 4.0. / Lucks, K. // Stuttgart: Schäffer-Poeschel Verlag. – 2017 [in German]
- Lux, T. E-Health – Begriff und Abgrenzung. In S. Müller-Mielitz & T. Lux (Eds.), E-Health Ökonomie (pp. 39-57). Wiesbaden: Springer Gabler.- 2017 [in German]
- Mathar, T. Der digitale Patient. Bielefeld: Transcript Verlag. – 2010[in German]
- Ministerstvo zdravoohraneniya RF [Russian Ministry of Healthcare (official site)]. [Electronic Resource] – URL: https://www.rosminzdrav.ru/ministry/61/22/informatsionnye-materialy-po-napravleniyu strategicheskogo-razvitiya-rossiyskoy-federatsii-zdravoohranenie/elektronnoe-zdravoohranenie (accessed: 10.06.2020). [in Russian]
- Programma «Cifrovaja jekonomika Rossijskoj Federacii» [Digital economy of the Russian Federation program]. [Electronic resource] – URL: http://static.government.ru/media/files/9gFM4FHj4PsB79I5v7yLVuPgu4bvR7M0.pdf 9gFM4FHj4PsB79I5v7yLVuPgu4bvR7M0.pdf (accessed: 14.03.2020). [in Russian]
- Postanovlenie Pravitelstv RF #447 [Decree of the Russian Government #447]. [Electronic resource] – URL: https://telemedicina.ru/news/law/pravila-deyatelnosti-medicinskih-organizacij-v-sfere-cifrovogo zdravoohraneniya, (accessed: 10.06.2020). [in Russian]
- Prikaz #268 o vvedenii v deystvie otraslevogo klassifikatora Slozhnyie i kompleksnyie meditsinskie uslugi. [The Decree #268 “On the Introduction of the Sectoral Classificator of Complex and Medical Services.”]. [Electronic resource] – URL: http://www.zakonprost.ru/content/base/25908 (accessed: 10.06.2020). [in Russian]
- Prikaz # 965 ob utverzhdenii poryadka organizatsii meditsinskoy pomoschi s primeneniem telemeditsinskih uslug. Utverzhden prikazom Ministerstva zdravoohraneniya RF. [The Prilozhenie 1 k Trebovaniyam k gosudarstvennyim informatsionnyim sistemam v sfere zdravoohraneniya sub'ektov Rossiyskoy Federatsii, meditsinskim informatsionnyim sistemammeditsinskih organizatsiy i sistemam farmatsevticheskih organizatsii [Appendix 1 to “Requirements for state health information systems of the constituent entities of the Russian Federation, medical information systems of medical organizations and information systems of pharmaceutical organizations.”]. [Electronic resource] – URL: https://telemedicina.ru/news/law/funktsionalnyie-vozmojnosti-gosudarstvennyih-informatsionnyih sistem-v-sfere-zdravoohraneniya-subyektov-rossiyskoy-federatsii (accessed: 10.06.2020). [in Russian]
- Vladzimirskij A.V. Telemedicina: Curatio Sine Tempora et Distantia. [Telemedicine: Curatio Sine Distantia et Tempora] // Moskva: Aegitas. – 2016 [in Russian]
- World Health Organization [Electronic resource] – URL: https://www.who.int/ehealth/en/ (accessed: 12.08.2020).