PSYCHOLOGICAL COUNSELLING IN TREATMENT FOR IN VITRO FERTLIZATION

Belevska J.1, Belevska D.2, Lutovska R. M.3
1Master of clinical psychology, medical doctor, PHI “Dr. Lozankovski”, Skopje; 2Doctor of social science, clinical psychologist, Dean of Faculty of psychology at ISU “G.R. Derzavin”, R. of Macedonia; 3 Master of neurology, psychologist, Centre for counseling and psychotherapy, Skopje
PSYCHOLOGICAL COUNSELLING IN TREATMENT FOR IN VITRO FERTLIZATION
Abstract
Own family is the essence of person’s life. Forming family is the most important life event, for the couples. Often, it’s planned precisely in details, as education or career. Failure in this plan causes variety of negative psychological consequences. That’s why infertility of one or both of the partners is a serious problem. In the treatment of biologically supported fertilization, negative emotions may affect the successfulness of the IVF treatment. Intending to overcome negative emotional reaction, this study aims to identify the efficiency of psychological counseling of candidates for IFV in stress, anxiety and depression decreasing, and the impact of counseling over the successfulness of the treatment. Method: Random sample of 64 candidates for IVF treatment in total are divided in two groups: control group without psychological counseling (32 candidates) and intervention group of 32 candidates included in psychological counseling. DASS scale is used to measure stress, anxiety and depression, semi structured interview is used to collect demographic and fertility data. Study results support the implementation of psychological counseling for candidates of IVF treatment.
Keywords: IVF treatment, stress, anxiety, depression, psychological counseling
Introduction
Own family is the essence of person’s life. Forming family is the most important life event, for the couples. Often, it’s planned precisely in details, as education or career. Failure in this plan causes variety of negative psychological consequences. That’s why infertility of one or both of the partners is a serious problem that causes emotional reactions, in each of them, that have negative impact on the successfulness of IVF treatment.
There have been a number of clinical reports on the emotional impact of IVF treatment. Infertility reflects over personal self confidence and it correlates with emotional responses as stress, depression, anger, guilt, frustration and sadness. Treatment failure appears to be associated with these emotional reactions [1,2,3,4,5,6].
Psychological counseling is one way to attempt to neutralize these reactions, or to decrease their impact over successfulness of the IVF treatment. The following tasks of counseling can be distinguished in the context of infertility treatment: information gathering and analysis, implications and decision-making counseling, support counseling and therapeutic counseling. It can be used before, during and due to end of the IVF treatment, aiming to help partners to overcome psychological barriers, as a serious threat of IVF treatment successfulness [7,8].
Infertility is defined as inability of a sexually active, non-contracepting couple (woman and man) to achieve pregnancy in one year [9]. Infertility includes psychological suffering, trauma and initiated need of professional help. First stop for solution are infertility clinics. Looking for medical diagnosis, couple faces with doctors efforts basically direct toward medical anomalies. Doctors dealing with medical problem inevitably faces with couple psychological problems [10]. They must be prepared to handle emotional and psychological doubts, based on the importance of their role in couple’s life in this period. At the beginning patients may respond to the doctor according to the relationship that they have mutually built. Furthermore, patients reactions may be predicted by early childhood and past life experiences that happened beyond doctor – patient relation [11,12].
Infertility can be painful and devastated experience for partners, man and woman, and their reactions are impacted by personal expectations. Strong wish for children and consecutive reactions toward infertility are defined by our culture trough complexity of personal, family, social and medical expectation that overcome sex, age, religion, ethnicity and socio-economic class [4].
Infertility is often secret life crisis, lived by the partners in isolation [1,2,3,4,5,6].
The aim of the study is to examine the impact of psychological counseling over decreasing of stress, anxiety and depression in candidates for IVF treatment, and to explore how counseling on the beginning of treatment affects on the successfulness of IVF treatment.
Method
The examined candidates were recruited from the Clinical hospital “Acibadem Sistina” Skopje. The sample comprised 64 randomly selected women, candidates for IVF treatment, divided in two groups: control group without psychological counseling (32 candidates) and intervention group of 32 candidates included in psychological counseling. An inclusion criterion for the study is infertility – primary or secondary. The psychometric instrument used for evaluation of stress, anxiety and depression was DASS scale.
DASS scale is multiple choices, self-reported inventory for measuring negative emotional reactions of depression, anxiety and stress. DASS is designed not only as a scale to measured conventionally defined emotional conditions, but also to lead the process of defining, understanding and measuring the omnipresent and clinically significant emotional states usually described as depression, anxiety and stress. Thus, the DASS should successfully meet the demands of researches and professional clinicians.
DASS integrated 3 scales with 14 items by scale, divided in subscales of 4 to 5 items with similar content. The Depression scale evaluates dysphoria, hopelessness, impairment of life, self humiliation, lack of interest/involvement, lack of will and inertia. Anxiety scale evaluates autonomic arousal, skeletal muscles effects, situation anxiety and subjective feeling of unspecified nervousness – anxiety. Stress scale is sensitive on levels of chronic nonspecific reactivity. The scale evaluates difficulty in relaxing, nervousness, condition of light agitation, irritability, hipper reactivity and intolerance. Examinees rates all of the items on scale with 4 levels of frequency, depending on what extend they experienced the described condition in the last week. Total scores for depression, anxiety and stress are calculating by summing the scores from the relevant items [13]. Data of fertility were obtained with protocol of semi structured interview with patients, as well as demographic data that relates with relevant variables (year of birth, place of birth, education, occupation, marital status, nationality). Both instruments were applied in the beginning of the IVF treatment.
Results
Study results confirm that: Psychological counseling of candidates for IVF can reduce the impact of stress, anxiety and depression among candidates and contributes to a greater success of treatment with IVF.
The results show that intervention group that was included in psychological counseling has statistically significant lower scores on stress (t=3,201, p<0,05) and anxiety (t=2,311, p<0,05). The scale of depression do not show statistically significant differences in the two groups compared.
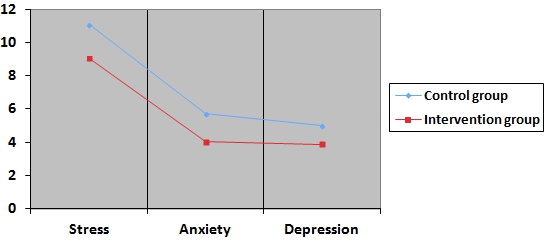
Fig. 1 - Scores on DASS for both groups
Using multiple tables and Chi square is found that the number of candidates from intervention group who are pregnant is statically significant bigger than the number of pregnant candidates from the control group.
Table 1 - Number of pregnant candidates from both groups
| Pregnant | Total | |||
| Yes | No | |||
| Psychological counseling | Yes | 22 | 10 | 32 |
| NO | 15 | 17 | 32 | |
| Total | 37 | 27 | 64 | |
χ²=4,625 df=1, p<0,05
Study results confirm that psychological counseling used in the beginning of the treatment with IVF has positive impact. Success of the treatment with IVF is more common among candidates that were included in psychological counseling. It can be seen from the Table 1. in the intervention group of 32 candidates that have been included in psychological counseling, after the treatment with IVF, 22 are pregnant, and from the control group out of 32 candidates who have been exposed to treatment with IVF without psychological counseling, only 15 are pregnant.
In relation of level of stress, anxiety and depression, candidates from intervention group who were undergoing psychological counseling, have lower middle scores than the middle scores of the candidates from control group without psychological counseling. This confirms the impact of psychological counseling on reducing stress, anxiety and depression and improved successfulness of the treatment with IVF.
Conclusion
Treatment of IVF has no long tradition in the R. of Macedonia, so there are not enough studies on this issue. Especially, there is a lack of studies concerning the psychological condition of candidates for IVF treatment. In the countries where IVF has longer tradition, the need for psychological and psychosocial support of candidates is clearly defined. Our study results confirm the importance of psychological counseling in the process of IVF treatment. Psychological counseling in the beginning of the IVF treatment decreases level of stress, anxiety and depression in candidates and affect over the successfulness of the treatment. Meaning that, our study results support the implementation of psychological counseling for candidates of IVF treatment.
References
- Menning E. The psychological impact of infertility. Nursing Clinics of North America. 1982; No. 17(1):155 -163.
- Sandelowski , Pollock C. Women’s experiences of infertility. Journal of Nursing Scholarship.1986; No. 18(2):140-144.
- Pearson Nursing Times.1992; No.88(3):36-38.
- Whiteford LM, Gonzalez L. Stigma: The hidden burdens of infertility. Social Science Medicine. 1995; 40(4):27-36.
- Schoener CJ, Krysa LW. The comfort and discomfort of infertility. Journal of Gynecological Neonatal Nursing.1996; 25 (5):167-172.
- Greil Infertility and psychological distress: A critical review of the literature. Social Science Medicine.1997; No.45 (6):1679-1704.
- Sharma V, Burt VK, Ritchie HL. Assessment and treatment of bipolar II postpartum depression: a review. J. Affect Discord.2010; 1(7).
- Sharma V, Burt VK, Ritchie HL. Bipolar II postpartum depression: Detection,diagnosis and treatment. Am.J.Psychiatry. 2009; 11.
- World Health Organisation. Recent Advances in Medically Assisted Conception, WHO Technical Report Series, 820, World Health Organisation Publ. 1992
- Берга С. Л, Пери Б. Л, Кирановски Џ. М. Психијатријата и репродуктивната медицина. Табернакул. 2012; 2, (1):2293-2315
- Lalos A. Breaking bad news concerning fertility. Human Reproduction. 1999; 14: 581-585.
- Kentenich H. Emotional Considerations within an Infertility Unit. Advances in Research in Psychosomatic Obstetrics and Gynaecology Parthenon. Carnforth. 1992; 551 – 556.