Клиническая характеристика пациентов со смешанным тревожным и депрессивным расстройством
Клиническая характеристика пациентов со смешанным тревожным и депрессивным расстройством
Аннотация
Смешанное тревожное и депрессивное расстройство представляет собой сложную коморбидность, характеризующуюся одновременным наличием признаков тревоги и депрессии у пациентов, что усиливает негативную симптоматику и осложняет процесс лечения. По отдельности невозможно выделить наиболее доминирующую категорию, что не позволяет поставить диагноз депрессивного расстройства или расстройства, связанного с тревогой и страхом. Анализ и исследование корреляции тревожных и депрессивных расстройств определяется разнородностью клинических проявлений и повышением суицидальных тенденций. Смешанное тревожное и депрессивное расстройство относится к группе невротических расстройств, основной характеристикой, которых является осознания наличия болезни и неспособность самостоятельно преодолеть беспокоящий фактор. В статье проанализированы клинико-психологические особенности пациентов с данным расстройством и представлены результаты диагностики проявления тревоги и депрессии. Полученные данные могут быть использованы в практической работе клинических психологов.
1. Introduction
Anxiety and depressive states are most common among patients with mental disorders. These manifestations belong to the group of neurotic disorders, the main characteristic of which is the awareness of the presence of illness, illness and inability to overcome the disturbing factor. S.N. Pavlinich notes that in 60-70% of cases there is mutual influence in the manifestations of anxiety and depressive states . Thus, the observed patients may have both anxiety and depressive symptoms.
Based on the International Classification of Diseases of the 10th revision, the diagnosis of "mixed anxiety and depressive disorder" (F41.2) occurs precisely in cases when symptoms corresponding to both anxiety and depression are detected, but there is no predominant condition . In the International Classification of Diseases of the 11th revision, the diagnosis of "mixed depressive and anxiety disorder" (6A73) belongs to the group of depressive disorders of the affective spectrum, in the class of psychological, behavioral and neuropsychological development disorders (06) . It is clarified that the symptoms have been observed for more than two weeks. The code 6A73b of the ICD-11 corresponds to the code F41.2 in the ICD-10.
A number of symptoms can be identified that make it possible to distinguish mixed anxiety and depressive disorder from other pathological conditions: deviant behavior, immunity to criticism, decreased self-esteem, insecurity, instability of the emotional sphere.
G.V. Pogosova draws attention to the fact that in most patients, anxiety disorder precedes a depressive state, in other words, for a long time patients are not diagnosed, therefore, anxiety is not treated, which is further aggravated by signs of depression .
O.S. Levin points out that anxiety and comorbid conditions, under the influence of constant stress, are a factor that increases the risk of a spectrum of neurodegenerative diseases .
Considering in more detail the anxiety disorder and the specifics of its manifestation, it should be noted that, unlike anxiety, characteristic of any person, this phenomenon has a more stable and long-lasting character.
Anxiety, as a property of the psyche, helps a person to beware of danger, not to commit rash acts, and is also an impetus for development. As noted by I.A. Golman, anxiety contributes to the operation of the "quick mind" mechanism, timely analyzing data from the outside world, reporting a perceived threat, causing emotional and behavioral responses . However, an increase in the level of anxiety has a negative impact on human life, constant dissatisfaction, instability of the emotional sphere, insecurity, a feeling of instability causes anxiety, therefore, prevents you from getting a positive, positive experience. Thus, anxiety is the body's response to the influence of external and internal factors and includes psychological, mental, somatic, and social components. In the practice of a clinical psychologist, a psychiatrist, the most common cases are an increase in the level of anxiety, rather than an unjustified decrease.
The increase in patients with neurotic anxiety disorders in modern society can be associated with an increase in the general level of dissatisfaction and tension, the need for multitasking and the speed of achieving goals, the dissemination of information, the imperfection of mechanisms of psychophysical adaptation and protection. I.A. Golman reports: "Patients and principals with an increased level of anxiety make up a significant percentage (in our practice – up to 30% and above) from all those seeking psychological help. And the more significantly this level is increased, the greater the emotional discomfort experienced by the owner of such a psyche" .
Analyzing the pathological appearance of anxiety, the following characteristics come to the fore: persistent or temporary unfounded doubts and suspicions, unreasonable excitement, expectation of adverse events, a state of internal tension, negative emotional and behavioral reactions, which contributes to impaired functioning in society, impaired adaptation and a decrease in the quality of life. Data from the World Health Organization indicate that 3.6% of the world's population is diagnosed with an anxiety disorder .
S.N. Pavlinich identifies concomitant pathological states of anxiety, so panic attacks with generalized anxiety occur in 56% of cases, obsessive-compulsive disorders in 35%, and social phobias in 32-42%. The comorbidity of generalized anxiety with depression varies from 23 to 87% .
It should be noted that in the theoretical study of D.Y. Veltischev and A.S. Marchenko, the delivery of the diagnosis of "generalized anxiety disorder" is questioned, since this condition, due to the nonspecificity of manifestations, occurs within the framework of acute neuroses, psychogenic reactions, with character accentuations and secondary psychopathies of an anxious-hypochondriacal type .
Analyzing such a phenomenon as a depressive episode or depressive disorders, it is possible to identify the main characteristics that appear in pronounced sadness and decline, which leads to a violation of human activity and loss of interest in the world.
N.A. Sosunova notes that there is a connection between the manifestations of a pathological depressive state and the time of the year, periods such as autumn and winter are especially significant. A change in the weather, a reduction in daylight hours, leading to changes in the rhythm of life, contributes to a change in mental state, anxiety, depression, drowsiness, lack of strength. These circumstances are aggravated by colds, affecting the physical condition of the patient .
E.A. Medvedeva studies the relationship between the level of depression and the somatic and psychosomatic status of a person and establishes that the disorder can be accompanied by various somatic diseases . Thus, a depressive episode may be accompanied by somatic changes: sleep disorders, daily routine or weight changes and cognitive manifestations: impaired concentration.
Thus, the diagnosis of "mixed curd and depressive disorder" according to ICD-10 or "mixed depressive and anxiety disorder" according to ICD-11 is characterized by the influence of anxiety depressive symptoms at a time for a period of two weeks. With increased anxiety and the understanding that the observed state of health is painful, a person plunges into an apathetic state, leading to depression. There are thoughts about not being needed, about one's own difference from the environment, about rejection in society, lack of support, which exacerbates the anxiety state. Depressive symptoms include a decrease in mood, deterioration of well-being, loss of aspirations and hobbies, and lack of a sense of well-being. The symptoms of anxiety are manifested in constant anxiety, expectation of failure, suspicion, the presence of a feeling of fear, internal tension, nervousness, increased irritability, psychoemotional tension with concomitant vegetative manifestations. Individually, it is impossible to single out the most dominant category, which does not allow the diagnosis of another depressive disorder or a disorder associated with anxiety and fear. It is accompanied by a pronounced feeling of discomfort, impaired functioning in society, impaired adaptation and a decrease in the quality of life.
2. Main results
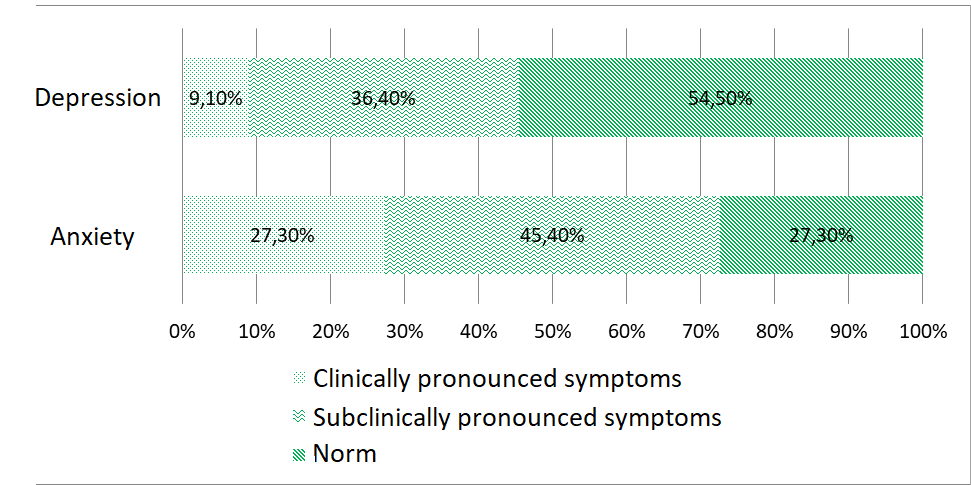
Figure 1 - Manifestation of anxiety and depression in patients with mixed anxiety and depressive disorder
It can be seen from the distribution that the majority of patients with mixed anxiety and depressive disorder are characterized by a norm, i.e. a low rate of depression (in 54.5%) and a subclinical severity of anxiety (in 45.4%), which indicates the presence of constant anxiety and agitation. The phenomena of an alarming series arise from the uncertainty and uncertainty that develops about the potentially dangerous situation of the disease.
Subclinical manifestations of depression predominate in 36.4% of the sample, and 9.1% have clinically pronounced symptoms of depression. Common to this group is a decrease in motivation and loss of interest in performing tasks that used to be enjoyable; loss of the ability to get satisfaction from the usual daily activities, and a decrease in the desire to do what you love.
27.3% of patients diagnosed with mixed anxiety and depressive disorder do not show a tendency to anxiety-related phenomena or excessive anxiety. However, negative thoughts and emotions can suddenly arise, affecting the overall well-being.
Clinically pronounced symptoms of anxiety are characteristic of 27.3% of patients in this sample, which indicates increased anxiety about their health and concern about the future, decreased motivation and loss of interest affect the adaptation of personality in the environment.
3. Conclusion
Thus, the majority of patients (54.5%) do not notice signs of depression in their own psychoemotional state, while 45.4% of patients with mixed anxiety and depressive disorder are characterized by the presence of anxiety symptoms at the subclinical level.
The obtained data can be used in the work of clinical psychologists in the preparation of psychological correction programs.