СТЕПЕНЬ УДОВЛЕТВОРЕННОСТИ ПАЦИЕНТОВ – ИНДИКАТОР КАЧЕСТВА МЕДИЦИНСКОГО СЕРВИСА

Шопов Д.Г.1, Михайлова В.К.2, Стоева Т.Р.3
1Кафедра социальной медицины и общественного здравоохранения медицинского университета, Пловдив, Болгария, 2Отделение профилактической медицины, факультет общественного здравоохранения, София, Главный ассистент кафедры управления здравоохранением, факультет общественного здравоохранения, Медицинский университет, Пловдив, Болгария, 3Университетская Больница Св. Георгия, Пловдив Болгария
СТЕПЕНЬ УДОВЛЕТВОРЕННОСТИ ПАЦИЕНТОВ – ИНДИКАТОР КАЧЕСТВА МЕДИЦИНСКОГО СЕРВИСА
Аннотация
Совместный анализ и оценка качества лечебно-диагностического процесса является необходимым условием для комплексного подхода к его управлению. Было изучено мнение пациентов, которые посетили и прошли лечение в клиниках университета многопрофильной больницы Св. Геогрия в Пловдиве. Для оценки их удовлетворенности качеством услуг здравоохранения в процессе лечения, была разработана анкета из 24 вопросов. Анонимное анкетирование подтверждает ряд закономерностей, связанных с качеством медицинских услуг. Основным моментом в оценке качества является ориентация на конечного потребителя – пациента, не исключая высокий уровень медицинских специалистов, параклинических и других вспомогательных элементов.
Ключевые слова: качество медицинских услуг, лечебно-диагностический процесс, пациент, удовлетворение.
Shopov D.G.1, Mihaylova V.K.2, Stoeva T.R.3
1MD, PhD, Chief Assistant Prof. Department of Social Medicine and Public Health Medical University, Plovdiv, Bulgaria, 2PhD, Assoc. Prof. Department of Preventive Medicine, Faculty of Public Health, Sofia, Chief Assistant Department of Healthcare Management, Faculty of Public Health, Medical University, Plovdiv, Bulgaria, 3Senior health care University Hospital “Sv. George” – Plovdiv Bulgaria
PATIENTS' SATISFACTION – AN INDICATOR OF THE QUALITY OF MEDICAL SERVICES
Abstract
The combined analysis and quality assessment of the diagnostic and treatment process is a precondition for an integral approach to its management, an issue which we shall try to review in the present article. For this purpose we studied the opinion of patients who have visited and have undergone treatment in the clinics of University Multi-Profile Hospital for Active Treatment „St. George“ in Plovdiv, regarding their satisfaction with the quality of the health services in the course of their treatment, by means of a developed questionnaire containing 24 questions. The anonymous questionnaire confirms a number of regularities related to the quality of medical services. The main point in the quality assessment is the focus on the end-user – the patient, without ignoring the high quality of medical specialists, paraclinical and supporting units.
Keywords: quality of medical services, diagnostic and treatment process, patient, satisfaction.
Introduction.
In the contemporary health system quality is an indisputable priority. Under the pressure of the daily practical needs in the last decade a series of scientific studies have been carried out with regard to quality analysis, assessment and management, including by Bulgarian authors (L. Ivanov, Zl. Petrova, Il. Batashki, D. Shopov).[1;2;4;5] This evidences not only the significance of the quality in healthcare but also the differentiation of a new independent scientific trend in the theory of health management – medical qualitology.[3;6]. The problems of medical qualitology are wide ranged and affect all spheres and aspects of the healthcare activity. Therefore the problem of healthcare management requires a wide integral approach, comprising all levels and elements of the health system. [7;8]
The procurement of high-quality hospital aid is an area which in the last years has gained wide popularity. This motivated scientists from all over the world to direct their research activity towards detailed study of the phenomena and processes evaluating the consumer satisfaction with the health services offered. [10:11]
The efficient quality management of the inpatients' aid considerably depends on the conceptual vision of quality as a concept and on the approaches to its evaluation.
The development and ratification of the contemporary concepts of quality can be conditionally differentiated into three main stages:
Stage 1 – the USA, the beginning of 1950s (W. Edwards Deming, Joseph M. Juran, Armand V. Feigenbaum, etc.)
Stage 2 – Japan, the end of 1950s (Kaoru Ishkava, Genichi Taguchi, Shigeo Shingo, etc.)
Stage 3 – New western wave, 1970s-1980s (Philip Crossby, Tom Peters, Klaus Moller, etc.)
According to W. Edwards Deming and Joseph M. Juran, the main tasks of the producers are to improve the process of creation and keep track of the customer demands. The cycle created by Deming (Plan – Do – Check – Act) formulates the principles for improvement of the quality.
Joseph Juran is the first to include the human aspect in quality management. His book „Quality Control Handbook“, issued in 1951, is still the main book for quality management.
Armand Feigenbaum is the founder of the thesis „Total quality control“.
He considers the quality control more as a business model, than as a technical tool.
The above stated stages in the development of the vision of quality in healthcare are the basis of the contemporary definitions of quality as a main concept in health management.
According to the concept of the World Health Organization, quality is the provision to each patient of sufficient types of diagnostic and therapeutic activities, ensuring best results with respect to health, in conformity to the achieved level of the medical science, at the best possible price for the same result, at a minimum iatrogenic risk and reaching the highest level of satisfaction with respect to procedures, results, humane treatment by the medical staff.
The definition given by the International Standardization Organization (ISO) treats quality as „A combination of specifications of a product or service, related to their ability to satisfy certain or preferrable needs“. The task of ISO is to urge the development of standardization and the related activities around the world, with a view to facilitation of the international exchange of goods and services.
The multi-factor dependence of the quality of health services is one of the reasons the issue of the criteria for its assessment to be still controversial to a certain degree. Most frequently the evaluation of quality is carried out through the scientific and technical level of the medical aid (medical technologies).[12:13]
The use of medical technologies as quality criteria in healthcare hides some conditionality, since they are an element at the entrance of the system; therefore they must always take into consideration the rest of the quality criteria, mostly pertaining to the exit from the system, i.e. the results of the healthcare services.[15]
The specific quality indicators are generally divided into two groups:
- Indicators of the quality of the process
- Indicators of the quality of the results.
The purpose of the present work is to study the opinion of patients who have visited and undergone treatment in clinics of University Multi-Profile Hospital for Active Treatment «St. George» - Plovdiv regarding their satisfaction with the quality of health services in the course of the diagnostic and treatment process. Materials and methods:
The collection, analysis and assessment of the results have been performed using sociological (questionnaire) and statistical methods. The survey was carried out among 409 patients who have visited the clinics of UMPHAT „St. George“ for the period July – September 2015.
A questionnaire containing 24 questions has been developed for the survey among the respondents. The questionnaire has been developed in strict compliance with the main principles of voluntariness and anonymity.
The questionnaire is direct, individual. The respondents fill in the questionnaire at a time suitable for them, put it in an envelope and seal it, after which they deliver the envelopes to the medical secretary of the relevant clinic. The participation is voluntary, with guaranteed anonymity and discretion. The computer processing of the collected database was carried out using the statistical package SPSS, version 19, and Microsoft Excel.
Results and discussions:
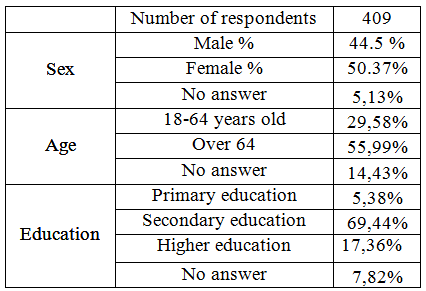
The survey was carried out among 409 patients at the age between 18 and 80, 29.58% of whom between 18-64 and 55.99% - over 64. The per cent of female respondents was 50.37% and the male ones – 44.5% (Table 1).
The educational level of the respondents was indicated, the majority of the patients had high school education (69.44%), followed by those with higher education (17.36%).
Table 1
The information about the direction of the patients to a medical institution and admission to hospital is represented on Chart 1. The highest relative share belongs to those directed towards hospitalization by their GP (55.26%), the second place is for patients who have been admitted at their personal choice (32.03%) and the last place is for those sent from another hospital (4.65%).
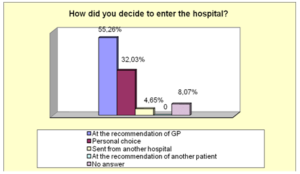
Chart 1
The patients have been divided into two groups, depending on the method of their admission to hospital – planned admission (38.88%) or urgently (56.97%) (Chart 2). The high per cent of those urgently admitted to hospital is impressive. Considering the time of the questionnaire (summer period), the patients prefer postponement of the planned treatment for the autumn. This is a natural process which has been observed in the previous years.
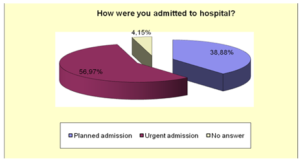
Chart 2
UMPHAT „St. George“ - Plovdiv is the biggest hospital in Southern Bulgaria. It has a high-tech equipment and very good specialists. It occupies a leading place on the market of medical services. This predetermines the large number of patients. 51.34% of the patients are admitted to the hospital for the first time, and 44.25% of the respondents indicated it as their preferred choice should they need subsequent medical treatment (Chart 3).
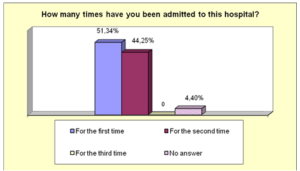
Chart 3
The knowledge of the Internal regulations of the clinic are important for the correct medical treatment of the patients. Right from their admission the patients must be familiarized with the daily routine and the internal rules. 94.38% of the respondents indicate a positive answer. An important place in their treatment is designated to the communicational skills of the medical staff. Since ancient times the father of medicine, Hippocrates has many times noted down that words have a healing power. The dialogue between the physician in charge and the patient about his health status is positive for 95.35% of the respondents. Information about the possibility for choice of a medical team and the price list of additionally required services of the clinic has been provided to 91.44% of the patients. In the course of the diagnostic and treatment process it was not necessary for the patients to purchase additional medicines or consumables from external sources. This was indicated by 95.11% of the respondents. The payment of a user fee is a mandatory element in the course of their stay in the hospital, with exception of those exempt due to particular indications. Payment for additional services or comfort at the medical institution was not necessary. An indicator of the quality of the outcome of the medical treatment is the satisfaction of 92.67% of the patients (Table 2).
Table 2
| Were you familiarized with the daily routine of the clinic? | yes | 94,38% |
| no | 5,62% | |
| Did your doctor in charge inform you about your condition? | yes | 95,35% |
| no | 0 | |
| No answer | 4,65% | |
| Were you familiarized with the prices of the additional services of the clinic? | yes | 93,40% |
| no | 6,60% | |
| Were you familiarized with your right to choose a team in the clinic? | yes | 91,44% |
| no | 0 | |
| No answer | 8,56% | |
| Did your relatives have to bring you medicines or consumables? | yes | 4,89% |
| no | 95,11% | |
| Did you pay for additional comfort or services in the medical institution? | Consumer fee | 80,93% |
| Fee for a VIP room | 0,98% | |
| other | 0 | |
| No answer | 18,09% | |
| Are you satisfied with your medical treatment? | yes | 92,67% |
| no | 0 | |
| partially | 0,73% | |
| I can't decide | 0 | |
| No answer | 6,60% |
Conclusion.
In the contemporary health systems quality occupies an indisputable priority. The anonymous survey carried out among patients treated in a large hospital confirms a number of regularities related to the quality of the medical services.
The constant transfer from good and high-quality provision to increased market release of the health product is in the basis of the dualistic nature of quality, which depends on the provider on the one side and on the user, on the other. The provider, according to his understanding, provides a high-quality product, which if not adapted to the customer demands, is not fit for sale. On the other side, the consumer with his demands specified by his purchasing capacity, is a determining factor for the provision of a high-quality product.
The provision and marketing of a hospital product of higher quality stimulates the separate hospitals to seek newer methods of treatment, combined with the best medical equipment and medical specialists.
The main point in the quality assessment is the focus on the activity of the end user — the patient, without prejudice to the high quality of the medical specialists, paraclinical and supporting units.
The constant improvement of quality includes assessment, activities and a new mental attitude for constant strive for excellent achievements. It consists of small steps, focuses on the process and is applied by people who work together. In healthcare the constant improvement of quality is used for the systematic study of methods of healthcare improvement. Subsequently the following results can be achieved:
- Improved health results of the patients.
- Increased satisfaction of the patient.
- Higher efficiency of the organization.
- Reduced costs.
References
- Hospital Management. Edited by L. Ivanov. 2005, 340 p
- Borisov V. The Hospital of the Future – Strategic Challenges. - Health Management magazine, 3, 2006.
- Kitov, B. Hospital Management — Theory and Current Approaches. Bulgarika Publishing House, 2003, 56 p
- Petrova, Zl., K. Chamov, St. Gladilov. Quality in Healthcare – Contemporary Dimensions and Tendencies. 2008, 270 p
- Shopov, D. Quality of Medical Service in Therapeutic Hospital Units. Dissertation paper, 2008, 181 p.
- Chamov, K. The Choice of Priorities in Healthcare – Principles, Practice, Techniques. - V: Petrova, Zl., K. Chamov, St. Gladilov. Quality in Healthcare – Contemporary Dimensions and Tendencies. 2008, 237-245 p.
- Belbin, M. Management team anatomy. London, 1990, 84.
- Donabedian A. Exploration in quality assessment and monitoring . The definition of quality and approaches to its assessment, Ann Arbor Health Administration Press, Vol 1, 1980; 30-50.
- Griffith, John R; White, Kennem R. The revolution in hospital management. - Journal of Healthcare Management, May 1, 2005.
- Jolly, D., I.Gerbaud. The hospital of tomorrow. WHO, Geneva, 56
- Mullins, L. Management and Organizational Behavior. Pitman Publishing, London, 1991, 545.
- Phillips, С et al. Evaluating Health and Social Care. Macmilan, London, 1994, 180.
- Rohme,K., L. Kjekshus. When time counts - hospital physicians use of time and work assignments. Tidsskr Nor Laegeforen, 2001, 121, 12, 1458-1461 (Record of Medline-R).
- Sauerland, D. The German strategy for quality improvement in health care: still to improve. Health Policy. 2001 May; 56 (2): 127-47
- Tchamov, K. Technology of priority setting in hearth policy. - In: Challenges of delivering hearth in the enlarged Europe -experience and perspectives from member states and associated countries. Proceedings, European Hearth Conference, Sunny Beach, Bulgaria 2006, 79-89.