СОВРЕМЕННЫЕ ПОДХОДЫ К ОЦЕНКЕ ЦИТОАРХИТЕКТОНИКИ ЭРИТРОЦИТОВ
СОВРЕМЕННЫЕ ПОДХОДЫ К ОЦЕНКЕ ЦИТОАРХИТЕКТОНИКИ ЭРИТРОЦИТОВ

Аннотация
В настоящей статье анализируются возможности применения микроскопических и иных методов оценки цитоархитектоники эритроцитов человека. В современной практической медицине широко используются данные, получаемые с помощью автоматических гематологических анализаторов. Указанные приборы обеспечивают высокую точность определения ряда гематологических показателей, в том числе количественную характеристику изменений размеров и формы эритроцитов — показатель анизоцитоза (RDW). Однако метод не позволяет визуализировать тонкие структурные изменения мембранной конформации клеток. Микроскопическое исследование мазка крови дополняет анализ гематологических сдвигов, обеспечивая более детальную оценку морфологических характеристик клеток. Прицельное изучение эритроцитарной морфологии может быть ограничено рядом факторов: вариабельностью методик пробоподготовки; особенностями фиксации клеток; влиянием поверхностного потенциала подложки на морфологию эритроцитов. Наиболее достоверные данные о минимальных изменениях цитоархитектоники эритроцитов предоставляют методы микроскопии высокого разрешения. Среди них особое место занимает сканирующая электронная микроскопия (СЭМ), позволяющая получить изображения с высоким пространственным разрешением. Ограничением широкого внедрения СЭМ в клиническую практику служит недостаточная оснащённость традиционных медицинских лабораторий электронными микроскопами, а внедрение световой микроскопии для целенаправленного изучения цитоархитектоники эритроцитов требует разработки специализированных протоколов пробоподготовки и проведения критической оценки качества получаемых результатов. В связи с этим перспективным направлением представляется использование высокоточных световых микроскопов с увеличением ×600 и более. Такие приборы способны дополнить и актуализировать данные гематологических анализаторов. Учитывая, что морфофункциональные изменения эритроцитов в различных микроокружениях представляют собой неотъемлемый компонент физиологического ответа организма на патогенетические воздействия, своевременная и точная оценка количественных и качественных характеристик этих клеток существенно повышает вероятность успешной коррекции нарушений гомеостаза.
1. Введение
The growing interest of researchers in erythrocytes is driven by their role in maintaining homeostasis at the level of the whole organism . An erythrocyte is one of the most important carriers of information about the state of tissue structures, as it has a lifespan of approximately 120 days. During this period, it circulates in the bloodstream and penetrates all organs and tissues, where it directly interacts with various stress‑inducing agents
, , .Mature erythrocytes lack the ability to synthesize proteins and, consequently, to repair cell damage after exposure to toxic agents. In diseases of various origins, there are typical non‑specific mechanisms of disruption to the molecular organisation of erythrocyte membranes. Cell death occurs not only in the immediate area of damage but also far beyond it, due to the activation of the apoptosis programme by tumour necrosis factors and inflammatory mediators . Currently, investigating the mechanisms of apoptosis activation is one of the most relevant and practically important tasks
, . Erythrocytes are unique cells that already include an apoptosis programme during their formation . In young cells, a high degree of integration between membrane structures and metabolic processes can be observed, ensuring optimal functioning. Once they enter the circulatory system, erythrocytes gradually disintegrate, which significantly affects the performance of vital functions: oxygen transport, adaptive functions, and possibly endocrine functions . Studying the mechanisms of erythrocyte disintegration allows for the development of more effective methods to protect cells and to correct emerging damage using targeted regulators and medications.Despite the fact that peripheral blood erythrocytes are one of the most suitable cellular models in the body, their investigation in practical medicine is not carried out comprehensively enough. This is due to the limited capabilities of existing tests, the complexity of modern equipment, and the lack of an integrated approach to interpreting the obtained parameters. Under the influence of physical and chemical factors that a person encounters in today’s environmental conditions and in their occupational activities, most changes in the function of the haematopoietic system are of an adaptive nature. Only in extreme cases are these changes a consequence of severe damage. It is difficult to identify and properly assess adaptive haematology responses to the effects of low‑intensity toxic factors. Minor changes in blood cell counts are easily “lost” among the physiological fluctuations inherent to these parameters, and the changes themselves are limited in their direction. Pathological changes in the blood are extremely diverse and depend not only on the severity of the process but also on the overall reactivity of the organism and any accompanying complications
, . Each method has its own specific features and limitations for use. However, knowledge of the nuances of operation and sample preparation allows for a competent approach to the analysis of the obtained results .2. Complete Blood Count and Haematology Analysers
Erythrocyte parameters such as morphology, volume, refractive index, and haemoglobin content are of great importance for diagnostic purposes . In practical medicine, clinicians traditionally rely on the complete blood count (CBC), which helps identify deviations in the body’s vital parameters. Today, a complete blood count includes the determination of approximately 30 tested parameters. Medical institutions are gradually moving away from routine manual methods for assessing the qualitative and quantitative composition of blood. Moreover, many characteristics of erythrocyte cells can only be detected using automated haematology analysers. Although blood morphology requires a comprehensive assessment, it is necessary to interpret each individual blood cell parameter, as each has its own clinical and diagnostic characteristics.
As a rule, a clinical blood test includes counting and determining the ratios of the main cellular populations of the erythrocytic, leucocytic, and thrombocytic lineages, taking into account the qualitative and quantitative composition of individual cell subpopulations and the width of their size distribution.
Regarding erythrocytes, the assessment of so‑called erythrocyte indices and the erythrocyte sedimentation rate is provided. Erythrocyte indices are calculated values that allow for a quantitative characterisation of important indicators of erythrocyte status :
1) RBC (red blood cells) — absolute erythrocyte count. There is a direct relationship between the number of erythrocytes in the blood and the mean corpuscular volume (MCV).
2) HGB (haemoglobin) — haemoglobin concentration in whole blood, determined photometrically using the cyanmethemoglobin or chromic methods.
3) HCT (haematocrit) — haematocrit level, reflecting the ratio of erythrocytes to blood plasma, expressed as a percentage.
4) MCV (mean corpuscular volume, HCT/RBC) — mean cell volume, measured in femtolitres (fL). Based on MCV values, anaemias are classified as microcytic, normocytic, or macrocytic.
5) MCH (mean corpuscular haemoglobin, HGB/RBC) — mean haemoglobin content per individual erythrocyte, measured in picogramms (pg).
6) MCHC (mean corpuscular haemoglobin concentration, HGB/HCT) — mean corpuscular haemoglobin concentration. This indicator reflects the haemoglobin saturation of an erythrocyte.
7) RDW (Red cell distribution width) — red cell size distribution width, an indicator of cell heterogeneity, expressed as a percentage.
8) RDW (%)=SD/MCV (fL)×100%, where SD is the standard deviation of the mean erythrocyte volume from the mean value.
9) RDW/SD — relative width of erythrocyte volume distribution, standard deviation.
10) RDW/CV — relative width of erythrocyte volume distribution, coefficient of variation.
11) ESR — erythrocyte sedimentation rate, a non‑specific indicator of a pathological condition in the body.
Depending on the type of haematology analyser and its operating principles (i.e., the diagnostic methods underlying it), minor variations in the reference values of the tested parameters may be obtained. These variations should be taken into account when analysing the clinical situation, especially when reviewing complete blood count parameters over time. Therefore, it is recommended to perform blood tests using the same equipment and taking into account the reference intervals of the given method. When interpreting the obtained data, one should rely not only on the average normal values but also on the individual characteristics of the reference intervals for the specific instrument. Erythrocyte indices determined by automated haematology analysers are of great importance for the differential diagnosis of anaemic syndromes and for monitoring the effectiveness of their treatment.
In relation to red blood cells, almost any automated haematology analyser is capable of generating a histogram — a curve showing the distribution of erythrocytes by volume. The shape of this histogram is used to assess the course of physiological and pathological processes in the body (Fig. 1).
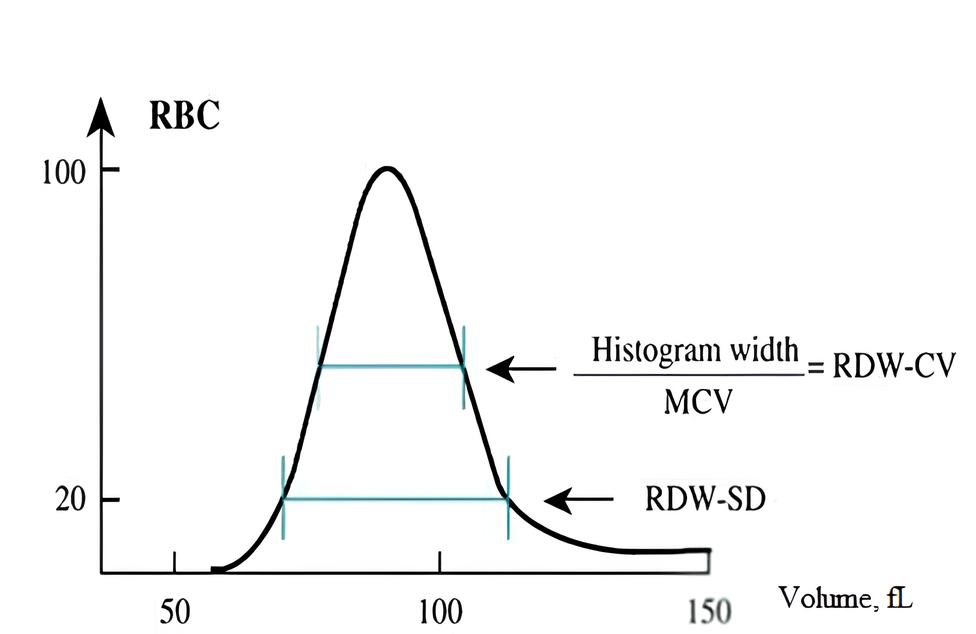
Red blood cell volume distribution curve
Haematology analysers detect anisocytosis significantly more effectively than visual methods. Assessing the degree of anisocytosis under a microscope is accompanied by a number of errors. When erythrocytes dry out in a blood smear, their diameter decreases by 10–20%; in thick smears, it is smaller than in thin ones. Numerical parameters of the complete blood count (CBC) such as RBC, MCV, and RDW are associated with the erythrocyte size distribution histogram. These parameters change in various haematology diseases and provide important information about the state of the erythrocytic component of haematopoiesis. However, an isolated assessment of these indicators is of limited informative value due to their averaged nature. The concentration of erythrocytes on the graph corresponds to the area under the distribution curve. The RDW SD parameter does not depend on MCV, so it better reflects the degree of anisocytosis in macrocytic conditions. Visual information obtained from studying the histogram provides a clear picture of the diversity of erythrocyte sizes and the predominance of certain populations. For a correct clinical interpretation of erythrocyte parameters, a comprehensive assessment of all indicators is necessary, combined with other laboratory data , .
3. Principle of Operation of Haemanalysers and Diagnosis of Pathological Conditions
Many haematological analysers operate based on impedance technology: the electric field created between two electrodes of opposite charge can be used to count cells and determine their size. Blood cells are poor conductors of electricity. The diluent in which they are suspended for passage through the orifice between the electrodes is an isotonic solution, which has good conductive properties. Accordingly, when cells suspended in the diluent pass through the orifice between the electrodes, the impedance (resistance) of the electric field between the electrodes momentarily increases for each individual cell. Each cell generates an electrical pulse proportional to its size. This is how the device determines morphological parameters , .
The use of automated haematological analysers is not limited to the diagnosis of anaemic conditions. For example, analysis of results from automated determination of complete blood count and electrolyte parameters has shown that an increase in the specific fluid content in an erythrocyte may accompany an adaptive response . Using automated haematology analysers, researchers have identified the clinical significance of laboratory parameters of the erythrocytic component of peripheral blood in the acute phase of schizoaffective psychosis, as well as in cases of herpesvirus and cytomegalovirus infections, and other conditions . Thus, numerous studies show that the use of the classical blood smear method can be successfully replaced by automated methods for determining clinical blood parameters , .
Modern haematological analysers make it possible to exclude morphological changes in cells caused by the use of a solid substrate, in particular, the influence of its surface potential on cytoarchitectonics
. Using automated analysers, one can not only assess the qualitative composition of cell populations but also determine the number of fragmented cells. However, despite its obvious advantages, this diagnostic method does not provide visualisation of the morphological picture of the erythron, which must be taken into account in a number of pathological processes of various etiologies. Changes in the cytoarchitecture of erythrocytes in response to pathogenetic influences serve as an important diagnostic parameter and reflect the cellular response at the level of the entire organism. Along with changes in the configuration of red blood cells, variations in their size, the ratio of transformed forms, shifts in haemoglobin content, and other processes are observed . Morphofunctional signs of erythrocyte “ageing” indicate impaired membrane elasticity and, consequently, the cells’ ability to undergo elastic deformation in the microcirculatory bed. In this context, it is relevant to study not only biochemical but also morphological parameters of cells using microscopy methods at various magnifications. Electron and optical microscopes are capable of reconstructing the three‑dimensional structure of cells in real time .4. Microscopic Examinations
A more detailed description of erythrocyte morphology — in particular, changes in their shape (ovalocytes, schizocytes, spherocytes, target cells, etc.), the presence of inclusions, the occurrence of nucleated erythrocytes, changes in colouration, and so on — is performed using microscopy. Reticulocyte counts are carried out in a separate test. Microscopic examinations of erythrocytes are an essential part of the basic assessment of the cytological picture of blood in the diagnosis of several diseases. Types of erythrocytic cells associated with anaemias have been characterised and classified using a logistic regression classifier: teardrop cells, echinocytes, acanthocytes, elliptocytes, sickle cells, and normal erythrocytes . In cases of haemolytic anaemias caused by mechanical damage to erythrocytes, schistocytes (fragmented cells) appear in the blood of patients. Their clinical and diagnostic significance lies in providing evidence of mechanical haemolysis of erythrocytes; however, their detection in blood is associated with several challenges
, , . The International Council for Standardisation in Haematology has developed recommendations for the identification of schistocytes. During counting, it is recommended to also take microspherocytes into account if other forms of schistocytes are present in the smear. Nucleated erythrocytes can be used as a marker of erythropoietic stress and help optimise transfusion therapy in patients with beta‑thalassaemia. It has been shown that the combined use of automated systems and manual microscopy in counting nucleated forms of erythrocytes can help optimise transfusion therapy for this group of patients. Assessing this parameter is considered more informative and effective than simply counting the absolute number of cells.Types of Microscopic Examinations
There are several types of microscopic examinations.
Photoacoustic microscopy allows for the preparation of 3D images of erythrocytes and enables mapping of the vascular network and tissue absorbers
. Force spectroscopy can be used to identify changes in the elastic properties of cells. Light microscopy helps detect impairments in the aggregation properties of erythrocytes when rouleaux (coin‑like stacks) are formed — particularly during prolonged storage of donor blood or when the conditions of the microenvironment change. Digital holographic microscopy can be applied to assess the impact of changes in various proteins (for example, ankyrin and flotillin‑2) on erythrocyte morphology . Phase‑contrast microscopy is used to detect erythrocyte deformability. It allows for the reconstruction of 3D cell images by measuring thermal fluctuations of membranes. Confocal microscopy can be employed to study the internal structure of erythrocytes, their individual molecules, and dynamic processes in membranes. Erythrocyte deformation is assessed using laser diffractometry. Scanning electron microscopy (SEM) provides insights into the features of cellular cytoarchitectonics , including cells’ ability to alter their conformation under the influence of various agents and microenvironmental conditions . In scanning probe microscopes, the study of surface microrelief is performed using specially prepared microprobes that essentially “feel” the object with an oscillating cantilever. A combination of expansion microscopy and single‑molecule localisation microscopy potentially allows achieving molecular resolution . For instance, it has been shown that the spectrin cytoskeleton in the region of indentations has a lower density and greater length than in the rim areas. This is direct evidence of cytoskeletal asymmetry in human erythrocytes .Currently, leukocyte count in peripheral blood can be determined using digital imaging combined with preliminary cell classification via artificial neural networks
. This approach allows for assessment of platelet and erythrocyte morphology and counting of their numbers. These systems are comparable in performance to traditional manual optical microscopy. However, it is important to note that they are designed to be used in collaboration with a qualified morphologist. This approach offers several advantages, including increased standardisation, efficiency, and the possibility of remote review. Quantitative phase imaging of erythrocytes (white‑light diffraction phase microscopy) can be used to obtain an interferogram of their surface. Traditionally, continuous wavelet transform using the Paul wavelet is selected to calculate surface profiles from the interferogram image . The quantitative Raman microscopy method is suitable for studying the biochemistry of erythrocytes at the subcellular level . The choice of research method is determined by its objectives and sample preparation conditions.5. Light Microscopy and Scanning Electron Microscopy
To analyse erythrocyte conformation using a light microscope, cells can be placed in a liquid nutrient medium or on a solid substrate, followed by staining with the Romanowsky–Giemsa method. This technique allows visualisation of various cell shapes, including those undergoing haemolysis — in the field of a light microscope, they appear as dark spots, known as erythrocyte “ghosts”. Cells of altered shape — echinocytes and stomatocytes — are also distinguishable and can be subjected to quantitative and qualitative analysis (Fig. 2).
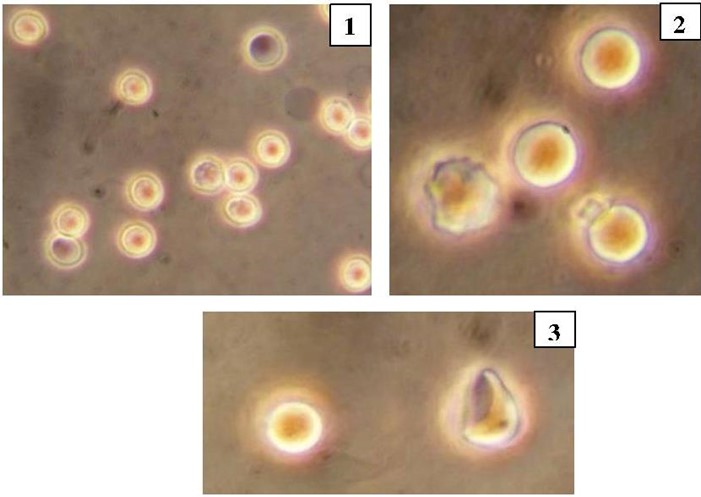
Human erythrocytes in a hypo‑osmotic NaCl solution (0,55 %)
1 — erythrocyte ghosts; 2 — echinocyte and discocytes; 3 — discocyte and stomatocyte
Photographic images obtained using a light microscope allow identification of the quantitative ratio of modified cells. However, they do not reflect the depth of variation in the cytoarchitecture of the samples. This goal can be achieved using scanning electron microscopy. Sample preparation of cells for analysis by scanning electron microscopy involves: fixation of erythrocytes with glutaraldehyde; drying in a series of aqueous ethanol solutions; coating with a thin gold film to improve the electrical conductivity of the samples. Electron micrographs of cells obtained using an electron microscope allow visualisation of surface changes in erythrocyte membranes — for instance, those induced by the presence of antibiotics in the incubation medium.
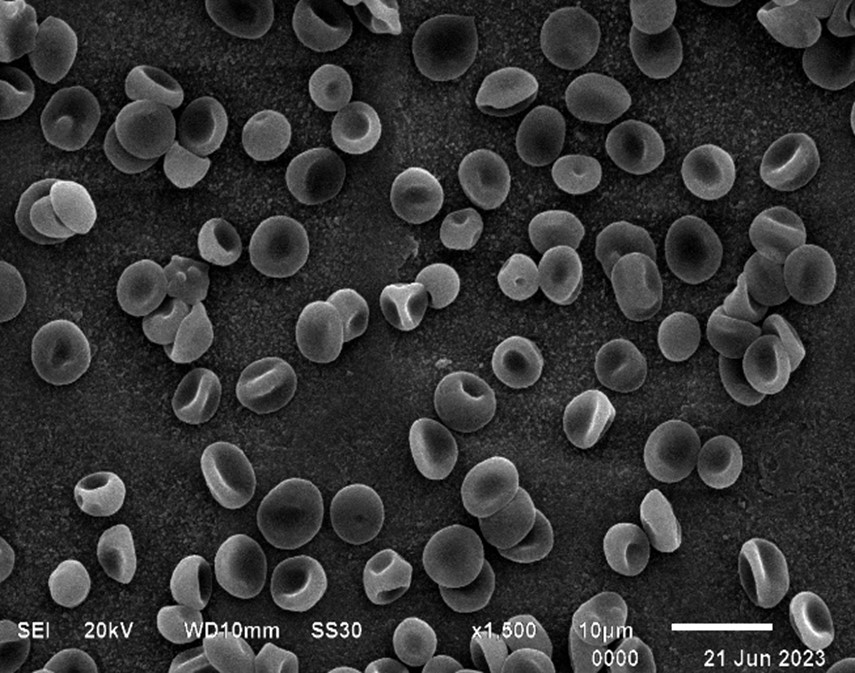
Scanning electron micrograph of human erythrocytes
When analysing the obtained data, researchers count reversibly and irreversibly transformed cell forms and identify features of the cell’s rotational figure — the pellor of erythrocytes — to establish differences between control and experimental samples. Knowledge of the ratio of normal to transformed cell forms allows for timely identification and monitoring of the progression of a pathological process.
6. Atomic Force Microscopy (AFM)
Assessment of the morphofunctional state of erythrocytes can also be performed using atomic force microscopy
. For example, a study of cell cytoarchitectonics in benign obstructive jaundice using AFM showed that as the severity of the disease increases, erythrocyte transformation occurs: the biconcave erythrocyte transforms into a dome‑shaped stomatocyte. There is a significant increase in erythrocyte volume, as well as an increase in the number and size of ruptures in the bilipid membrane layer . It has been found that patients with iron‑deficiency anaemia exhibit a significant number of elliptocytes, microcytes, stomatocytes, and spherocytes, which negatively correlate with haemoglobin concentration. Serum iron levels and total iron‑binding capacity strongly correlate with microcytes and the mean haemoglobin concentration in blood plasma. AFM has revealed noticeable disruption of membrane topology and increased roughness in these patients. The redox balance, assessed by reduced antioxidant capacity of plasma and intracellular levels of reactive oxygen species (ROS), is significantly impaired. In the erythrocytes of these patients, increased intracellular secretion of Ca2+ and phosphatidylserine is observed .Moreover, the development of a new morphological parameter for assessing the state of erythrocytic cells is of great importance. In particular, the introduction and use of plasma membrane roughness as a morphometric parameter has been described. By probing the cell surface at the nanoscale, atomic force microscopy (AFM) enables the study of the relationship between structure and function in both normal and pathological cells, and allows monitoring of specific morphological defects that arise in erythrocytes as intermediate stages following one another along the ageing pathway
, .A method for studying native blood cells using AFM in a humid chamber has been proposed and tested. This approach allows preserving the viability, size, and shape of biological objects. The method offers clear advantages over scanning, as it enables investigation of unfixed blood samples in the form of a suspension of living cells, thereby eliminating the impact of mechanical and chemical factors on them
. The surface characteristics of erythrocytes are important determinants for distinguishing thalassaemic cells. Both scanning electron microscopy (SEM) and AFM allow investigation of morphological deformations of erythrocytes in thalassaemias. In this case, AFM enables the most comprehensive study of the topographic characteristics of abnormal erythrocytes. The advantages of AFM are that this method not only allows obtaining high‑resolution images of living objects but also enables: studying cells in their native environment in real time; determining the viscoelastic properties of membrane‑cytoskeleton complexes; assessing the adhesive characteristics of molecules; and, in the long term, determining the local potential of cell membranes . Using AFM, one can obtain highly accurate morphometric characteristics of molecules, supramolecular complexes, and cells. Measurements of diameter and height allow relying not only on subjective information about changes in cell structure but also provide their precise quantitative assessment.When performing their basic physiological functions, erythrocytes undergo deformation. However, alongside physiological cell deformation, under adverse conditions erythrocytes transform into pathological forms that are not normally observed. It has been shown that the AFM method allows highly accurate measurement of cell height, diameter, and fractal dimension. However, the only highly sensitive parameter that enables differentiation of normocytes from transformed erythrocyte forms based on morphometric measurements is the fractal dimension
.Extracorporeal Pharmacotherapy
Accounting for the possibility of transformational changes in cells is also necessary when using erythrocytes as a means of drug delivery in the human body
, . Erythrocytic cells are promising carriers for a wide range of drugs and other biologically active agents. The main feature and advantages of erythrocytes as a drug delivery vehicle are their absolute biocompatibility and ability to circulate in the body for a long time. The internal environment of erythrocytic cells is relatively inert, protecting the delivered drug from inactivation by various endogenous factors. There are various methods for loading drugs into erythrocytes, based on the cells’ ability to undergo reversible transformation: electroporation; induced endocytosis; osmotic pulse haemolysis method; hypotonic haemolysis. Drug incorporation into erythrocytes can also occur naturally through sorption onto the cell membrane. Extracorporeal pharmacotherapy using erythrocytes as carrier cells is applied in the treatment of a wide variety of diseases. The range of drugs used and the opportunities provided are already quite broad, and further development of this direction holds great promise. Therefore, knowledge of the effects of any transported substance on erythrocyte morphology enables prediction of the success of the therapy and assessment of the likelihood of adverse effects.7. Conclusion
Thus, assessment of erythrocyte cytoarchitectonics can be performed using various research methods, each of which has its own level of sensitivity and error. Microscopic methods allow investigation of the spatial organisation of erythrocyte membranes, including possible changes in their microvesiculation, invaginations, and rearrangement of the central part of cells (the pellor). The state of red blood cells and their functional capabilities depend on the structural organisation of their membranes. Cell morphology and membrane nanostructure are compositionally and functionally linked to the cytoskeleton network. Features of erythrocytic architectonics, as well as identification of fragmented erythrocyte regions at appropriate magnification of a scanning microscope, open new perspectives in analysing the characteristics of cell morphological structures. Data obtained using microscopy methods can be taken into account when selecting an appropriate therapeutic strategy and in timely monitoring of the pathological process, aiming to minimise undesirable reactions. Modern approaches to assessing the surface architectonics of erythrocytes are extremely diverse. The choice of research method is primarily determined by its objectives, the availability of the method, and the possibility of result reproducibility.