Влияние экстремального возраста (100+ лет) на расхождения между формулами BIS1, MDRD и CKD-EPI при оценке СКФ у женщин
Влияние экстремального возраста (100+ лет) на расхождения между формулами BIS1, MDRD и CKD-EPI при оценке СКФ у женщин

Аннотация
Глобальное старение населения обусловливает необходимость точной оценки функции почек у лиц экстремального возраста (100 лет и старше). Существующие расчётные формулы скорости клубочковой фильтрации (СКФ) — MDRD и CKD-EPI — не были валидированы в данной возрастной группе, что создаёт риск гипердиагностики хронической болезни почек (ХБП) или недооценки её истинной тяжести.
Цель исследования: установить характер и величину различий между показателями СКФ, рассчитанными по формулам BIS1, MDRD и CKD-EPI, у женщин-долгожительниц в возрасте 100 лет и старше.
Из базы данных столетних жительниц Челябинской области отобрано 45 записей (женщины, возраст 100–108 лет). Для каждой пациентки на основании уровня креатинина сыворотки рассчитаны значения СКФ по трём формулам: BIS1, MDRD и CKD-EPI. Проверка нормальности распределения выполнена с помощью критерия Шапиро–Уилка. Сравнение наборов данных проведено с использованием t-критерия Стьюдента. Для анализа частот стадий ХБП применяли χ²-тест с поправкой Бонферрони для множественных сравнений. Статистическая обработка выполнена в среде Google Colab (Python, библиотеки pandas, numpy, scipy).
Медиана (95% доверительный интервал) СКФ составила: для BIS1 — 37,48 (35,24–40,79) мл/мин/1,73 м²; для MDRD — 53,73 (48,59–59,58); для CKD-EPI — 49,64 (44,71–54,82). BIS1 даёт значимо более низкие значения по сравнению с MDRD и CKD-EPI (p<0,001), тогда как MDRD и CKD-EPI статистически не различаются (p=0,162). По классификации ХБП: BIS1 не выявляет пациентов в стадии G2 (0% против 35,6% у MDRD и 20,0% у CKD-EPI) и классифицирует 75,6% пациентов в стадию G3b, тогда как MDRD — 20,0%, CKD-EPI — 33,3%. После поправки Бонферрони (α=0,00417) значимые различия сохраняются для сравнений BIS1 vs MDRD и BIS1 vs DPI по стадиям G2 и G3b.
У женщин столетнего возраста формула BIS1 даёт наиболее консервативные, но, вероятно, более точные оценки СКФ по сравнению с MDRD и CKD-EPI, которые систематически завышают фильтрационную функцию. Для клинической практики у пациенток 100+ лет предпочтительно использование BIS1; при его недоступности результаты MDRD и CKD-EPI следует интерпретировать с осторожностью.
1. Introduction
Due to global population aging, the problem of accurately assessing kidney function in individuals of extreme age is becoming increasingly important. The number of long‑lived individuals (persons aged 90 years and older) is steadily increasing worldwide, necessitating the development of specific approaches to the diagnosis and treatment of age‑associated diseases, including chronic kidney disease (CKD) , .
Assessing kidney function in the elderly presents a complex clinical challenge. On the one hand, physiological aging is accompanied by a natural decline in glomerular filtration rate (GFR) averaging 7–10 mL/min/1.73 m² per decade after the age of 30–40 years. On the other hand, the widely used estimating formulas — MDRD (2002) and CKD‑EPI (2009) — were developed in younger populations and have not been validated in patients older than 70 years. This creates a risk of both overdiagnosis of CKD (when applying general threshold values mechanistically) and underestimation of true kidney function decline , .
Centenarian patients represent a unique study population, as they exhibit all the features and characteristics of extreme aging. However, none of the existing formulas for estimating GFR have been validated in this age group .
The present study contributes to addressing this problem by providing data on the nature and magnitude of discrepancies between the BIS1, MDRD, and CKD‑EPI formulas specifically in centenarian women — a group that remains virtually unrepresented in the international scientific literature. This work provides a basis for selecting the most appropriate formula for clinical practice when managing patients of extreme age.
The results of this study have direct practical implications for geriatricians, nephrologists, and internists who care for long‑lived individuals. An evidence‑based choice of formula for GFR estimation can optimize the diagnosis of CKD, risk stratification, and treatment decisions in this most vulnerable patient population.
Aim. To determine the nature and magnitude of differences in GFR values calculated using the BIS1, MDRD, and CKD‑EPI formulas in female centenarians.
2. Research methods and principles
For this study, 45 records of female centenarians were extracted from a database assembled during the study “Evaluation of the medical and social status of hundred-year centenarians in the Chelyabinsk region” (Chelyabinsk region, Russian Federation). The extracted data included information on age, sex, anthropometric parameters, and venous blood creatinine levels .
Glomerular filtration rate (GFR) was then calculated using three creatinine‑based formulas: BIS1, MDRD, and CKD‑EPI (DPI).
The normality of the three resulting eGFR datasets was tested using the Shapiro–Wilk test; all three datasets were found to follow a normal distribution. Student’s t‑test was used to compare the datasets.
To compare the frequencies of chronic kidney disease (CKD) stages, the χ² test was applied, and Bonferroni correction was used to control for type I error in multiple comparisons.
All statistical analyses were performed in the Google Colab environment using the Python programming language, with the following libraries: pandas, numpy, scipy, and scipy.stats.
The study was approved by the Ethics Committee of the Medical and Psychological Institute of the South Urals (Protocol No. 5 dated 01.06.2026). All study participants gave their informed consent for the processing of personal data in accordance with the Federal Law of the Russian Federation “On Personal Data” No. 152‑FZ of 27.07.2006.
3. Main results
The analysis included 45 female centenarians aged 100 to 108 years (median age 101 years). For all patients, eGFR was calculated using three formulas (BIS1, MDRD, and CKD‑EPI [DPI]) based on serum creatinine levels (mean value 98.7 μmol/L).
All three sets of eGFR values followed a normal distribution according to the Shapiro–Wilk test (BIS1: W = 0.986, p = 0.847; MDRD: W = 0.981, p = 0.667; DPI: W = 0.980, p = 0.616). Descriptive statistics are presented in Table 1.
Table 1 - Main descriptive statistics of eGFR (mL/min/1.73 m²) for the three formulas
Parameter | BIS1 (n=45) | MDRD (n=45) | CKD‑EPI (n=45) |
Mean ± SD | 38.4 ± 7.4 | 54.9 ± 14.0 | 50.8 ± 13.4 |
Median (Q1–Q3) | 37.5 (33.8–42.5) | 53.7 (45.4–61.8) | 49.6 (41.9–57.6) |
95% CI for median* | 35.2 – 40.8 | 48.6 – 59.6 | 44.7 – 54.8 |
Min – Max | 22.6 – 55.6 | 26.7 – 88.1 | 24.1 – 83.4 |
Figure 1 presents box plots of the eGFR distribution for the three formulas. It can be observed that BIS1 has the smallest spread of values and is shifted toward lower values.
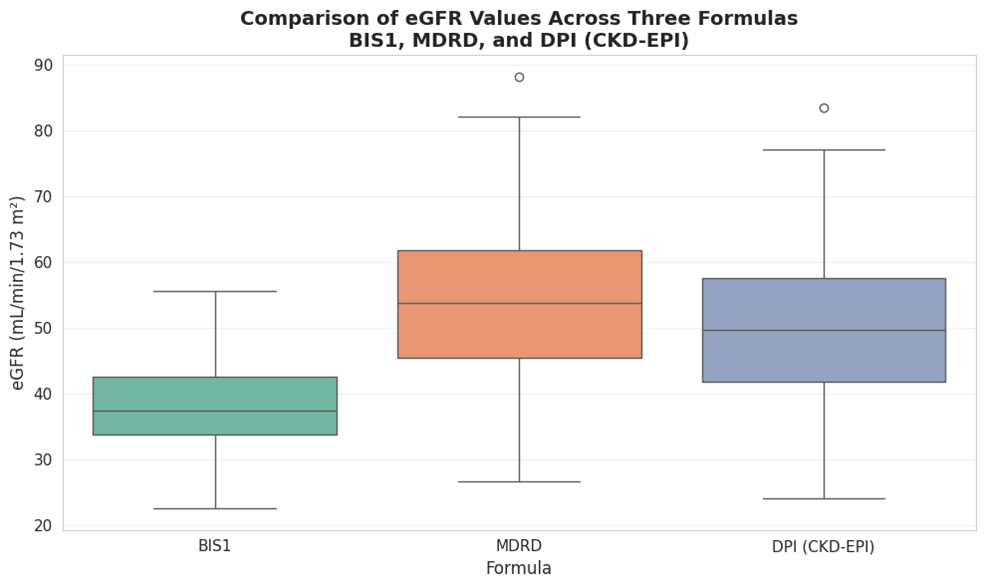
Comparison of eGFR Values Across The Formulas BIS1, MDRD and CKD-EPI
The BIS1 formula yields systematically lower eGFR values:
· BIS1 vs MDRD: mean difference = –16.49 (p < 0.001) — statistically significant
· BIS1 vs CKD‑EPI: mean difference = –12.42 (p < 0.001) — statistically significant
· BIS1 estimates eGFR approximately 25–30% lower than the other two formulas
MDRD and CKD‑EPI do not differ statistically.
Thus, the BIS1 formula provides systematically lower, but likely more accurate, eGFR values in centenarian women compared to MDRD and CKD‑EPI, which do not differ from each other and overestimate kidney function.
Applying the chronic kidney disease (CKD) classification, we examined the data obtained from the three groups. Based on the calculated eGFR values, patients were stratified into CKD stages. Stages G1 (≥90) and G5 (<15) were not observed with any of the formulas — see Figure 2.
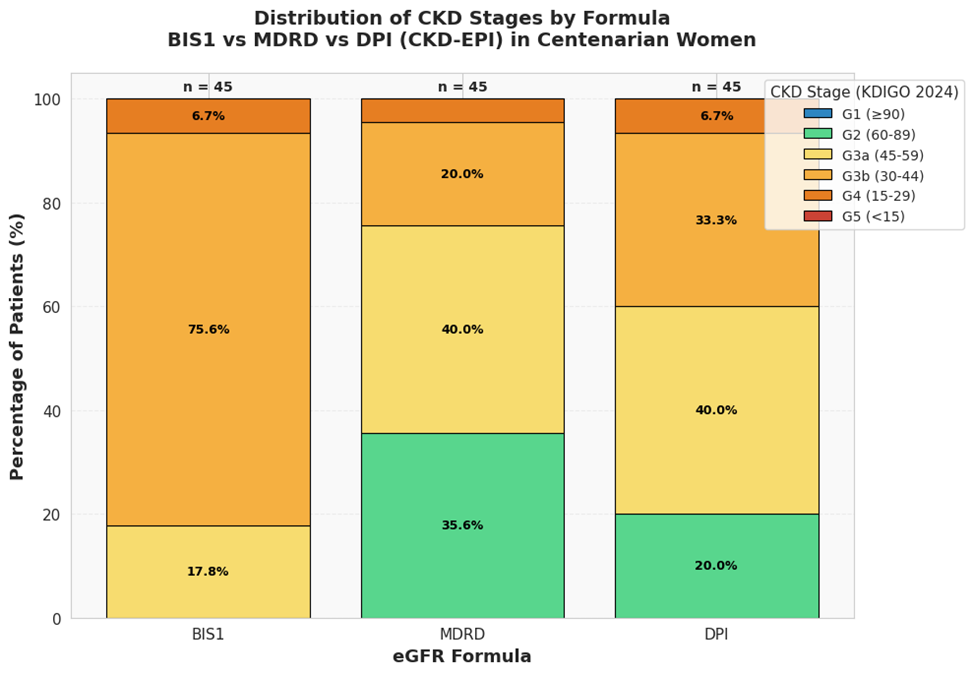
Distribution pf CKD Stages by Formulas
Key observations:
– BIS1 (the most conservative formula):
· 0% of patients in stage G2 (normal / mildly decreased);
· 75.6% of patients in stage G3b (moderate to severe decrease);
· Only 17.8% in G3a and 6.7% in G4;
– MDRD:
· 35.6% of patients in stage G2 — significantly higher than BIS1 and DPI;
· 40.0% in G3a — predominant stage;
· 20.0% in G3b;
– DPI (CKD-EPI):
· 20.0% of patients in stage G2;
· 40.0% in G3a — predominant stage (similar to MDRD);
· 33.3% in G3b;
To assess the significance of differences in the frequency of each stage between the formulas, a χ² test (2×2 contingency tables) was performed. Considering four stages and three pairwise comparisons (12 comparisons in total), Bonferroni correction was applied: α = 0.05 / 12 = 0.00417.
After correction, statistically significant differences were found only for stages G2 and G3b in the comparisons BIS1 vs MDRD and BIS1 vs DPI.
Results after correction:
1. G2: BIS1 vs MDRD — p = 0.000010.
2. G2: BIS1 vs DPI — p = 0.001565.
3. G3b: BIS1 vs MDRD — p = 0.000000.
4. G3b: BIS1 vs DPI — p = 0.000058.
The comparisons MDRD vs DPI did not reach significance for any stage (p > 0.05). For all other pairs (including all comparisons involving MDRD and DPI with each other), the differences did not reach the corrected significance threshold (p ≥ 0.020).
In women aged 100+ years, the BIS1 formula yields significantly lower and less variable eGFR estimates compared to MDRD and CKD‑EPI, which do not differ from each other. Accordingly, BIS1 classifies patients into more severe CKD stages (predominantly G3b), whereas MDRD and DPI often overestimate the category (G2–G3a). The observed differences are statistically significant (p < 0.001 for the means, and for stage frequencies after Bonferroni correction).
4. Discussion
The present study revealed substantial discrepancies in eGFR estimates between the BIS1, MDRD, and CKD‑EPI formulas in centenarian women. Our results are consistent with numerous international studies, confirming that the choice of estimating equation critically affects the classification of CKD stage in patients of extreme age.
Systematic underestimation of eGFR by BIS1. In our study, the BIS1 formula provided the most conservative eGFR estimates: the mean value was 38.4 mL/min/1.73 m², which is 16.5 mL/min/1.73 m² lower than that obtained with MDRD. Similar results were reported in an Italian study of 499 patients older than 70 years (mean age 82.6 years), where BIS1 estimated eGFR on average 13 mL/min/1.73 m² lower than CKD‑EPI and MDRD .
The study by Koppe et al. (2013) in 224 patients older than 70 years using direct inulin clearance measurement (the gold standard) showed that BIS1 has the lowest variability (SD 9.21 vs. 12.78 for MDRD) and the highest accuracy (P30 75.56% vs. 70.67% for MDRD). These data confirm that BIS1 not only yields lower eGFR values but does so with greater precision in elderly patients .
Comparison of MDRD and CKD‑EPI. An important finding of our work is the absence of statistically significant differences between MDRD and CKD‑EPI (p = 0.162). Our mean values (54.9 and 50.8 mL/min/1.73 m², respectively) are close to those of the Italian study (70.9 and 70.5 mL/min/1.73 m²), although the absolute numbers are higher, which may be explained by the younger age of their cohort (mean age 82.6 years vs. 100+ years) . With advancing age, the gap between BIS1 and the other formulas widens, as confirmed by Han et al. (2020) in a cohort of 966 centenarians .
Comparative accuracy of formulas in old age. A Chinese study from 2024 in 298 elderly patients (mean age 71 years) confirmed that BIS1 demonstrates the best accuracy compared to MDRD and CKD‑EPI . This pattern holds true for centenarian patients in our study as well.
Analysis of CKD stage distribution. Stage G2 (60–89 mL/min/1.73 m²). The most striking difference was observed for stage G2: BIS1 classified no patient into this category, whereas MDRD did so in 35.6% and DPI in 20.0%. These differences remained statistically significant after Bonferroni correction (p = 0.00001 and p = 0.0016, respectively). This indicates a systematic overestimation of eGFR by the MDRD and CKD‑EPI formulas, leading to a “rejuvenation” of kidney function in centenarians.
In the work by Vega and Huidobro (2021), it is noted that overestimation of eGFR by MDRD and CKD‑EPI in the elderly leads to an artificial down‑staging of CKD, which may deprive patients of necessary treatment . In the context of centenarian patients, this is particularly critical because the risk of drug accumulation and nephrotoxic effects increases manifold.
*Stage G3b (30–44 mL/min/1.73 m²).* The predominance of BIS1 in the G3b category (75.6% vs. 20.0% for MDRD and 33.3% for DPI) with highly significant differences (p = 0.000000 and p = 0.000058) is a key finding. The Italian researchers also noted that with increasing age, BIS1 shows a consistent decline in eGFR, whereas MDRD and CKD‑EPI do not exhibit such a trend . This indicates that the general formulas do not account for the physiological age‑related decline in kidney function.
Hahn and Strutz (2024) remark that for a 90‑year‑old patient, an eGFR value of 32 mL/min/1.73 m² formally corresponds to stage G3b CKD, but considering age‑adjusted norms it could be regarded as normal. However, KDIGO has not yet adopted age‑adapted thresholds; therefore, using BIS1 in centenarians is the most justified approach.
Stages G3a and G4. For stage G3a (45–59 mL/min/1.73 m²), the differences between BIS1 and MDRD/CKD‑EPI were significant before Bonferroni correction (p = 0.020) but lost significance after adjustment. This is explained by the fact that with four multiple comparisons, the significance threshold is lowered to 0.004, and the effect, though present, does not reach this stringent criterion.
For stage G4 (15–29 mL/min/1.73 m²), no statistically significant differences were found. The low absolute frequencies (2–3 patients) limit the statistical power of the comparisons; nevertheless, it is clinically important to note that BIS1 identified slightly more patients in this severe category (6.7% vs. 4.4% for MDRD).
Clinical implications. The clinical significance of the correct choice of formula goes beyond statistical differences. Overestimation of eGFR may lead to:
1. Underscoring of CKD stage and consequently the lack of timely nephroprotective therapy;
2. Overdose of renally excreted drugs (especially dangerous in patients with polypharmacy);
3. Inaccurate prediction of the risk of progression to kidney failure.
Study limitations and future research directions.
Our study has several limitations:
1. Relatively small sample size (45 patients);
2. Study of a female‑only population;
3. Lack of data on cystatin C.
Promising future directions include: prospective studies with direct measurement of GFR in centenarians, validation of combined formulas (BIS2, CKD‑EPI 2021 with cystatin C) in the 100+ age group, as well as investigation of the association between formula choice and clinical outcomes (hospitalisation, mortality, CKD progression).
At the same time, the results of the present study are consistent with data from other major works examining approaches to eGFR assessment in the population of long-lived individuals. The main distinguishing feature of the present study was the age of the participants: 100 years and older , .
5. Conclusion
1. There are statistically significant differences between the BIS1, MDRD, and CKD‑EPI formulas in estimating GFR in centenarian women. BIS1 provides the most conservative eGFR estimates (mean 38.4 mL/min/1.73 m²), whereas MDRD and CKD‑EPI yield higher values (mean 54.9 and 50.8 mL/min/1.73 m², respectively).
2. Pairwise comparisons with Bonferroni correction (α = 0.00417) revealed significant differences in the frequency of stages G2 and G3b between BIS1 and the other two formulas: — G2: BIS1 vs MDRD (p = 0.00001), BIS1 vs DPI (p = 0.00157) — G3b: BIS1 vs MDRD (p = 0.00000), BIS1 vs DPI (p = 0.00006) — MDRD and DPI did not differ for any stage (p > 0.05 for all comparisons).
3. BIS1 classifies 75.6% of patients into stage G3b (moderate to severe GFR reduction), whereas MDRD classifies only 20.0% and DPI 33.3% into this stage. Moreover, BIS1 identifies no patients in stage G2 (normal / mildly decreased), in contrast to MDRD (35.6%) and DPI (20.0%).
4. Our results are consistent with international studies in elderly patients (Koppe et al., 2013; Italian study 2024; Chinese study 2024), confirming that BIS1 has the lowest variability and the highest accuracy in the age group over 70 years. The only large study in centenarians (Han et al., 2020, n=966) also demonstrated that the formulas are not interchangeable, and that BIS1 is preferable for elderly women with low creatinine levels.
For clinical practice in women aged 100 years and older, the BIS1 formula is preferable, because MDRD and CKD‑EPI systematically overestimate GFR, which may lead to underestimation of CKD stage, inaccurate prognosis, and risk of drug toxicity. When BIS1 is not available, results from MDRD and CKD‑EPI should be interpreted with caution, taking into account their tendency to overestimate GFR in centenarians.