СИНДРОМ ДИСПЕРСИИ ПИГМЕНТА. МИКРОСТРУКТУРНЫЙ АНАЛИЗ В ЕСТЕСТВЕННЫХ УСЛОВИЯХ

Иванчева В.
ORCID: 0000-0001-6077-4639, кандидат медицинских наук, кафедра офтальмологии и визуальной науки, медицинского университета - Варна, Болгария
СИНДРОМ ДИСПЕРСИИ ПИГМЕНТА. МИКРОСТРУКТУРНЫЙ АНАЛИЗ В ЕСТЕСТВЕННЫХ УСЛОВИЯХ
Аннотация
Цель работы состоит в том, чтобы продемонстрировать в естественных условиях лазерную софокусную микроскопию как возможность для точного диагноза и контроля роговой оболочки при синдроме дисперсии пигмента, включая динамические микроструктурные наблюдения. В естественных условиях лазерная софокусная микроскопия демонстрирует новые перспективы для диагностики синдрома дисперсии пигмента (PDS). У метода есть более широкие возможности для контроля и долгосрочного прогноза.
Ключевые слова: синдром дисперсии пигмента, софокусная микроскопия в естественных условиях.
Ivancheva V.
ORCID: 0000-0001-6077-4639, MD, PhD, Department of Ophthalmology and Visual Science, Medical University - Varna, Bulgaria
PIGMENT DISPERSION SYNDROME – MICROSTRUCTURAL ANALYSIS IN VIVO
Abstract
The purpose of this work is to demonstrate in vivo laser confocal microscopy as an option for precise diagnosis and monitoring of the cornea in pigment dispersion syndrome, including dynamic microstructural observations. In vivo laser confocal microscopy demonstrates new perspectives for diagnostics and staging of the pigment dispersion syndrome (PDS). The method has wider applications for monitoring and long term prognosis.
Keywords: pigment dispersion syndrome, in vivo confocal microscopy
In vivo confocal microscopy facilitates optical slicing throughout the living cornea and provides imaging at cellular level [1]. This technology has led to a better understanding of the cellular microstructure in health and disease, enabling quantitative and qualitative analysis of the human cornea in vivo. There are number of studies dedicated to corneal nerves, stromal keratocite density and endothelial characteristics of the normal human and ageing cornea. However, in the literature there are diverse papers describing different pathological observations.
The main purpose of this study is to describe and measure number of characteristics of the patient with PDS using in vivo confocal microscopy. PDS is a relatively rare condition that leads to secondary open angle glaucoma, most common amongst young male myopes [2, 3]. Pigment dispersion syndrome is an ocular condition characterized by dispersion of iris pigment throughout the eye. PDS can be associated with ocular hypertension or glaucoma and is usually bilateral [3].
The purpose of our study was to describe the structural changes of the cornea in patients with pigment dispersion syndrome and to demonstrate in vivo laser confocal microscopy opportunities for precise diagnosis and long term monitoring. Twenty patients (40 eyes) between the age 35- 60 years, 5 female and 15 male with clinical signs of PDS were selected for the purpose of the study. Each eye was examined with slit-lamp biomicroscopy, goniscopy, fundoscopy and in vivo laser confocal microscopy. Microstructural assessment was focused on quantity and quality of subbasal nerve plexus, endothelial cells and morphology of the pigment granules. Laser scanning in vivo confocal microscopy was performed using the Heidelberg Retina Tomograph 3 Rostock Corneal Module (RCM); Heidelberg Engineering GmbH. Corneal confocal microscopy were performed using standard protocol. For each cornea three images were selected from the following levels: basal epithelium, sub basal nerve plexus, anterior stroma, mid stroma, posterior stroma and endothelium. Collected data were analyzed independently by 2 investigators using the same criteria.
Results
The study highlighted changes at three different levels: epithelium, sub-basal plexus and endothelium (fig 1). At superficial level the most prominent observation was the changing morphology of the basal epithelial cells in correlation to clinical stage of the disease. In advanced cases, especially associated with increased IOP, epithelial mosaic was irregular with presumed oedema at this level (fig 1 row A). Sub-basal nerve plexus also demonstrated pleomorphic morphology, however with advancement of the pigmentation, the nerves appear to decrease in density and increase in diameter. Also change in morphology was noted as looping and beading (fig 1 row B).
Corneal stroma had less prominent change but generally with advancement of disease we encountered decreased number of keratocytes (fig 1 row C). A correlation between the clinical characteristic and the degree of polymegathism and pleomorphism of affected endothelial zones was also observed. Quantitative analysis found a mean density of the pleomorphic endothelium to be 698 ± 74 cells/ mm². However the peripheral endothelium appears to be normal with density 2200 ± 56 cells/ mm². This observation was clinically undetectable. The most significant findings are hyper-echogenic, polymorphic granules on the back side of endothelial cells, measured 21 µm ±13, corresponding to the IOP. The size and density of the granules in patients with high intraocular pressure was significantly enlarged (fig 1 row D).
In the literature there are limited number of case studies describing PDS and glaucoma using in vivo confocal microscopy, and specifically HRT3 for morphometric analysis [4, 6]. Our study demonstrated new perspectives for diagnostic the pigment dispersion syndrome. The observations would have monitoring and prognostic advantage and differential diagnostic value with conditions associated with clinically similar pigment deposits on the back surface of the cornea over the endothelium. In our study we described changes in nerve morphology, which differs from other observations. The most prominent feature was thickening of the nerves in advancement of disease. As the patients had no history of any other ocular or systemic disease, nor prior cataract surgery, we believe that this is related to the syndrome. Whether this is an isolated nonspecific finding or whether thickened nerve plexuses may be more frequent in patients with PDS requires further observations in longer follow up over few years.
In some cases, uveitis can cause pigment epitelitis of the iris with release of pigment, inflammatory cells and debris behind endothelium. After resolution of the inflammation clinical observations might be mistaken for PDS [5]. We believe that polymegathism and pleomorphism in PDS are localized in the area of Kruckenberg spindle and the rest of endothelium is relatively normal. That could be an important diagnostic characteristic for differentiation of other conditions.
PDS is an important often underdiagnosed condition because it affects young people with potential risk of irreversible blindness. Confocal microscopy may not only detect pigment particles in early stages when impossible to be observed by slit lamp biomicroscopy, but also precisely measure the size and record changes in morphology. Furthermore this technique allows observation at microstructural level of all corneal levels and precise follow up of the dynamic changes in epithelium, sub-basal plexus and endothelium. Therefore, eye specialist may rely not only on precise diagnose but may utilize prognostic characteristics and utilize those for follow up.
Laser scanning in vivo confocal microscopy provides a novel method for examining microstructural alteration in PDS in the cornea, as well as other subclinical corneal pathology. The study demonstrated ability of in vivo laser confocal microscopy for diagnostics of PDS, including staging. The method has wider applications that are still to be developed and utilised for monitoring and long term prognosis.
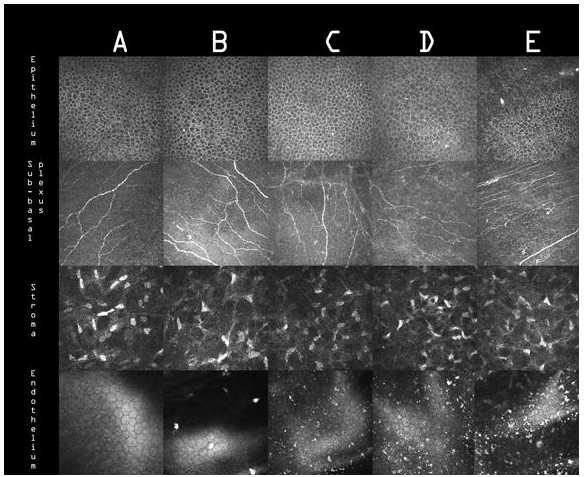
Figure 1 - Confocal microscopy at different levels of the cornea affected by PDS: epithelium (A), subbasal nerves (B), stroma (C) and endothelium (D). The columns are demonstrating the specified levels for healthy cornea and corneae with mild, moderate and advance development of the PDS as well in case with pigmentary glaucoma.
References
- Erie JC, McLaren JW, Hodge DO, et al. The effect of age on the corneal subbasal nerve plexus. Cornea 2005;24:705–9.
- 2. Niyadurupola , Broadway D. Pigment dispersion syndrome and pigmentary glaucoma, a major review. Clinical and Experimental Ophthalmology 2008; 36: 868–882.
- 3. Campbell DG, Schertzer RM. Pathophysiology of pigment dispersion syndrome and pigmentary glaucoma. Curr Opin Ophthalmol 1995; 6: 96–101.
- Peeva S, T Marinova, V. Ivancheva et al. Pigment dispersion syndrome - how to utilize in vivo laser confocal microscopy. Trakia journal of sciences 2012, Vol 10, 2, 133-137
- Dua HS, Dick AD, Watson NJ, Forrester JV. A spectrum of clinical signs in anterior uveitis. Eye 1993; 7: 68–73.
- Angelov B, Toshev A. Confocal laser-scanning ophthalmoscopy in diagnostics ot primary open angle glaucoma. Bulgarian forum glaucoma 2012; 2(1):20-29