ОСОБЕННОСТИ ПСИХОЛОГИЧЕСКОГО СТАТУСА И КАЧЕСТВА ЖИЗНИ ЖЕНЩИН С ХРОНИЧЕСКОЙ ИШЕМИЕЙ МОЗГА НА ФОНЕ МЕТАБОЛИЧЕСКОГО СИНДРОМА В ПЕРИОД МЕНОПАУЗЫ

Чичановская Л. В.1, Сергеева Е.Н.2, Бахарева О.Н.3
1 Доктор медицинских наук, зав. кафедрой генетики Тверского ГМУ, 2 аспирант кафедры неврологии нейрохирургии и медицинской генетики Тверского ГМУ, 3 кандидат медицинских наук, ассистент кафедры генетики Тверского ГМУ
ОСОБЕННОСТИ ПСИХОЛОГИЧЕСКОГО СТАТУСА И КАЧЕСТВА ЖИЗНИ ЖЕНЩИН С ХРОНИЧЕСКОЙ ИШЕМИЕЙ МОЗГА НА ФОНЕ МЕТАБОЛИЧЕСКОГО СИНДРОМА В ПЕРИОД МЕНОПАУЗЫ
Аннотация
В статье рассмотрено – изменение структуры головного мозга, и психологического статуса у женщин в периоде менопаузы, в зависимости от наличия метаболического синдрома, необходимость применения превентивного лечения у данной категории лиц.
Ключевые слова: менопаузальный синдром, хроническая ишемия мозга, метаболический синдром, инсулинорезистентность, депрессия, тревога, качество жизни.
Ciechanowski L.V.1, Sergeeva E.N.2, Bakhareva O.N.3
1 MD, 2 Postgraduate student, 3 MD, SBEI HVE Tver SMA Ministry of Health of the Russian Federation
PSYCHOLOGICAL STATUS AND QUALITY OF LIFE FEATURES OF WOMEN SUFFERING FROM CHRONIC CEREBRAL ISCHEMIA ASSOCIATED WITH METABOLIC SYNDROME IN THE PERIOD OF MENOPAUSE
Abstract
The changing structure of the brain and the psychological status of women in menopause, depending on the presence of a metabolic syndrome, and the need for preventative treatment for this category of people are discussed in this article.
Keywords: menopausal syndrome, chronic cerebral ischemia, metabolic syndrome, insulin resistance, depression, anxiety, quality of life.
According to the World Health Organization (WHO) 42% to 50% of all patients visiting a neurologist fall into the group of psychosomatic patients [1]. There is a number of pathologies in which the role of psychosomatic interections during the development and course is extremely high [2]. It is established that menopause, irrespective of age, is a trigger factor of development and progression of emotional and personal problems. Abnormalities in psychoemotional sphere are typical for such diseases as chronic cerebral ischemia. Also metabolic syndrome presence within this category of patients (which is in its turn connected to insulin resistance (MS) [5], dislipidemy and hyperpiesis) promotes formation of the "vicious" circle leading to development of vascular accidents [3, 4]. The central nervous system is extremely sensitive to insulin, that is a factor of sympathetic nervous system activation, vascular tone increase, arterial hypertension (AH) progression, CCI intensity growth.
The metabolic syndrome is a late sign of menopause since it is caused by serious metabolic disorders in the body, affected by a sharp shift of the endocrine profile. Female reproductive hormones deficiency with the increased level of steroid hormones in adrenal glands causes changes in metabolic processes, carbohydrates and fats. Without adequate compensation, glucose intolerance with subsequent development of insulin resistance advances, that in turn leads to the triglycerids’ level increase, the most modified class of lipids, and antiatherogenic cholesterol and high-density lipoprotein decrease. By the same token that leads to the increase in arterial pressure and formation of prerequisites for cardiovescular diseases. [6]. The significance of mental factors and psychophysiological interaction when having these pathologies can be discussed from three positions: causative factor, metabolic disorder and as a reaction to a disease and necessity in an independent treatment. The progressive course of CCI with the appearance of micro- and macrovascular complications and high disablement reduces the quality of life of these patients [7]. The assessment of the latter is used in applied medicine as the criterion allowing to receive information on the physical, psychoemotional and social condition of a person, that is especially important in the course of treatment of chronic pathology [8].
Objective: to estimate the psychological status and quality of life of women during menopause, suffering from chronic cerebral ischemia with the signs of metabolic syndrome.
Materials and methods of research
257 women in physiological menopause (average age 47,9±2,4 years) were examined. 127 of them underwent ambulatory treatment for CCI, and 80 patients had no signs of CCI.
All patients underwent general physical examination, that included collecting medical history and anthropometric measures: body weight, height, waist measurement (WM, cm) and hips measurement (HM, cm), with the subsequent calculation of the body weight index (BWI, WHO) and the ratio WM/HM. Also laboratory diagnostics were conducted: determination of the glucose level (mm/l), cholesterol (mole/l), estradiol (pg/ml), progesterone (nnmole/ml), with calculation of body mass index (BMI)
Methods of functional diagnostics included: duplex scanning of brachiocephalic vessels, brain MRI.
The study of the psychological status of patients consisted of identification of anxiety and depressive disorders by means of Spilberger-Khanin’s technique. Situational anxiety (PX-1) and personal anxiety (PX-2) were evaluated. Anxiety intensity was defined as follows: normal range - the score didn't exceed 30, moderate anxiety – 31 to 45 points; and severe anxiety - 46 and more points. The presence and severity of depression (light – 10-15 points, moderate - 16-19 points, heavy - 20-29 points, severe - ≥30 points) were diagnosed on Beck's scale. The assessment of patients' quality of life indicators was made by means of MOS SF-36 questionnaire on eight scales, that included physical functioning (Physical Functioning – PF), role functioning caused by physical condition (Role-Physical Functioning-RP), intensity of pain (Bodily pain - BP), general state of health (General Health - GH), vital activity (Vitality - VT), social functioning (Social Functioning – SF), role functioning caused by emotional state (Role-Emotional – RE), mental health (Mental Health – MH).
Statistical data processing was performed using the package of the applied statistical program Statistica 6.0. Results are presented in the form of mean value and standard deviation (M±σ). To validate the results and hypotheses Student's t-test and Pearson's "chi-squared" test were used. The presence of the interaction and its direction were determined by conducting a correlation analysis using Spearman test (r).
Results and their discussion
Depending on the signs of MS patients were divided into three groups. The first (main) group consisted of 127 women in physiological menopause (average age 50,7 ± 3,36 years), who had CCI and MS (BMI 31±5,29 kg/sq.m , WM - 101±16,04 cm, WM/HM - 1,00±0,14). The second group (control group 1) included 80 patients (46.8±12,45 years, p1<0,05) without signs of CCI, but suffering from MS (BMI 36,4±6,67 kg/sq.m; p1<0,05; WM–102.5±12,64 cm, WM/HM-0,84±0,08; p1<0,05) and having signs of hyperglycemia (blood glucose 5.36 mmol/l). 50 patients (47.8±5,56 years, p3,0.05) without organic brain damage and without metabolic disorders were assigned to the third group (control group 2) (BMS 22.7±3,23 kg/sq.m; p2<0,05, WM - 76,3±11,72 cm; p2,3<0,05, WM/HM-0,82±0,06; p3<0,05).
The age of the disease according to the medical history in all groups didn't differ significantly and averaged from 10,2±6,53 (group 1) to 11,1±9,32 years (group 2). Fasting glycemia in patients with CCI was significantly higher then in control groups (6,9±2,47 mm/l against 5,36±0,78 mm/l in the 1st group; p1<0,05 and 4,8±0,67 mm/l in the 2nd group; p3<0,05).
Symptoms of chronic cerebral ischemia (CCI) were found in 100% of cases in the I (main) group studied, this is reflected in the following figures. Thus, CCI in the 1 stage was detected in 36% of cases (45.7 people), CCI in the 2nd stage in 60% (76.2 people). During the analysis of a hypertensive disease the distribution was in favor of AH of II stage – 69% of the control group 1, then distributed further as follows: AH I stage – 22%, AH - III stage – 5%.
The analysis of the psychological status showed the presence of anxious and depressive symptoms in all patients.
Situational anxiety, according to the questionnaire, was widespread in all groups with a predomenance of its moderate levels (in 62-79% of cases). The average PX-1 values in groups didn't significantly differ (respectively 42,6±7,25 points, 34,0±7,63 and 38,1±6,17 points). Situational anxiety was more pronounced in patients with CCI and MS.
When assesing the personal anxiety (RX-2), its wide distribution was revealed in all groups, especially in women with MS without signs of CCI. Patients of the main group had anxiety in 45,32% of cases. Patients from both control groups had it in 100% of cases. Average values of personal anxiety accounted 43,7±10,1 points in the main group, 50,7±6,10 (p1<0,01) in control group 1 and 51,5±6,87 points (p3<0,01) in control group 2. Severe anxiety in patient groups without CCI (comparison groups 1 and 2) occured in 51.5% of cases respectively, that was significantly more often than in patients in group 1 – (χ ² = 14,0; p1<0,005 and χ ² = 12,3; p3<0,005).
The study of depressive symptoms showed opposite trends. The prevalence of depression according to Beck's scale was obtained in patients with CCI. It occured in 93% of cases. At the same time 56,9% was diagnosed with depression in control group 1, 47,5% of women and in control group 2 (χ ² = 8,9; p3<0,005).
Light and moderate depression dominated in most examined patients, that was indicated by median values on Beck's scale (1,6±9,12 points in the main group, 11,0±5,9 points in the control group 1, 12,0±8,19 points in the control group 2; p1,3<0,05). At the same time heavy and severe depression was much more often diagnosed in patients from control groups 1 and 2, those states were detected in 17.9% and 18.3% of patients (χ ²= 9,8; p1<0,005 and χ² = 8,1; p3<0,005). As CCI progressed, severity of depression decreased - 9.3%
Thus, anxiodepressive syndrome is widespread among women in menopause and is more pronounced with CCI and MS. At the same time there is a certain evolution of the syndrome components severity with a predominance of anxiety, both situational, and personal, in the early stages of the process and a decrease in depressive simptoms as CCI progresses. The presence and growth of MS, acompanied by worsening of the disease, appears to be crucial for the develompent of situational anxiety, while personal anxiety is more dependent on other factors. Its decrease in patients with CCI can be connected, on the one hand, with the development of organic changes in the brain, and on the other hand, with age-related changes [10].
The prevalence of depression in patients with CCI and MS evidences serious consequences of chronic cerebral ischemia, that also occur at the level of the psycho-emotional state. In addition, it leads to difficulties in successfully treating both patients with CCI, as well as with MS without corresponding psychiatric correction.
Quality of life assesment on scales of SF 36 questionnaire revealed that quality of life is reduced in women who suffer from CCI and MS (tab. 1).
Table 1. Indicators of quality of life in women in menopause with MS and CCI (main group), against the background of MS (control group 1) and no signs of MS (control group 2) (М±σ)
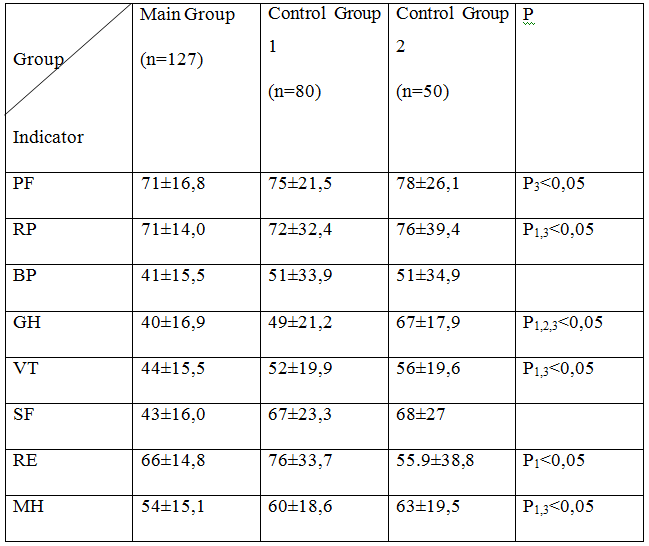
Notes: the difference between the groups - P1between the main group and control group 1; P2 between control group 1 and control group 2; P3 between the main group and control group 2.
This is evidenced by lower values on the scales of physical and role functioning, vitality, general and mental health of the surveyed main group, control groups 1 and 2. Peruliarities of CCI progression in the presence of MS also affected the quality of life of these patients. The psychological state of patients wth CCI was linked with their quality of life.
Thus, the CCI in women against the background of age-related changes in the female body reduces physical and psychoemotional components of the quality of their life. That is connected, on the one hand, with peculiarities of the disease (chronic cerebral ischemia), and on the other, with participation of symptome group in menopause genesis, including vascular, neuropsychological, metabolic and endocrine disorders. [4, 10].
CCI in patients with MS is associated with reduced quality of life to a greater extent on the scale of physical component. That could be explaind primarily by large BMI of patients. Depression also has a certain impact on the decline in the quality of life of all examined people.
Thus, anxiety, both personal and situational, is mostly typical in patients without CCI, whilst situational anxiety is higher in patients with MS. Depression is mostly diagnosed in patients with CCI and its severety rises with increasing BMI and decompensation of their disease. It affects the quality of life of patients, both with CCI and with MS. The presence and severety of MS, especially in patients with CCI, substantially disrupts the quality of life of women, reducing their physical and role functioning, worsening their general and mental health, vitality and emotional role. The quality of life of women in menopause with the most evident MS also decreases on scales of vitality, role functioning, the general state of health.
References
- Gusev, E.I. Ishemija golovnogo mozga [Tekst] / E.I. Gusev, V.I. Skvorcova. – M.: Medicina, 2007. - 254 s.
- Malkina-Pyh I. G. Psihosomatika: Spravochnik prakticheskogo psihologa, 2005. - M.: Izd-vo Jeksmo, - 992 s.
- Kondakov I.M. Psihologija. Illjustrirovannyj slovar'. - 2007. – SPb.: Prajm-EVROznak, – 783 s.
- Mychka V.B., Bogieva R.M., Chazova I.E. Akarboza – sredstvo profilaktiki mnozhestvennyh serdechno-sosudistyh faktorov riska metabolicheskogo sindroma // Klin. farmakol. i ter. – 2003. – № 12(2). – S. 80 № 3.
- Chazova I.E., Mychka V.B. Metabolicheskij sindrom // Kardiovaskuljarnaja terapija i profilaktika. – 2003. № 3. – S. 32-8
- Kondakov I.M. Psihologija. Illjustrirovannyj slovar'. - 2007. – SPb.: Prajm-EVROznak, – 783 s.
- Adasheva T. V., Demicheva O. Ju. // Lechashhij vrach.- 2003.- № 10.- S. 24-28.
- World Health Organization – International Society of Hypertension. Guidelines for the Management of Hypertension. J. Hypertension 1999; 17 (2): 151-183; 30(Suppl. 2): 1-7.
- Ackroff K., Sclafani A. Effects of the lipase inhibitor orlistat on intake and preference for dietary fat in rats. Am J. Physiol, 1996; 271(1Pt2): R48-54.
- Alberti K.G., Zimmet P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med, 1998; 15 (7): 539-53.
- Alessi M.C., Perietti F., Morange P., Henry M., Nalbone G., Juhan-Vague I. Production of plasminogen activator inhibitor 1 by human adipose tissue: possible link between visceral fat accumulation and vascular disease. Diabetes, 1997, May; 46(5): 860-7.