СТРАТЕГИЯ ПРОФИЛАКТИКИ И ЛЕЧЕНИЯ ПОСЛЕОПЕРАЦИОННОЙ ФИБРИЛЛЯЦИИ ПРЕДСЕРДИЙ
Дембеле А.1, Пастухова Н.К. 2
1Аспирант, 2Доктор медицинских наук, Санкт-Петербургский государственный педиатрический медицинский университет, Россия.
СТРАТЕГИЯ ПРОФИЛАКТИКИ И ЛЕЧЕНИЯ ПОСЛЕОПЕРАЦИОННОЙ ФИБРИЛЛЯЦИИ ПРЕДСЕРДИЙ
Аннотация
В статье рассматривается – Тактика профилактики и лечения фибрилляции предсердий при аортокоронарном шунтировании (АКШ), выполненном в разные периоды от начала инфаркта миокарда. Изучается эффективность раннего назначения бета-адреноблокаторов (метопролол) и амиодарона (в профилактических дозах) для снижения риска развития фибрилляции предсердий в послеоперационном периоде (период после проведения аортокоронарного шунтирования) у разных групп пациентов. А также анализируется эффективность применения дигоксина для купирования эпизодов постоперационной фибрилляции предсердий.
Ключевые слова: Аортокоронарное шунтирование (АКШ), профилактика, фибрилляция предсердий.
Dembele A.1, Pastukhova N.C.2
1Postgraduate student, 2MD, Saint-Petersburg State Pediatric-Medical University
STRATEGIES OF PROPHYLAXIS AND MANAGEMENT OF POSTOPERATIVE ATRIAL FIBRILLATION
Abstract
This article analyses different strategies of prophylaxis and management of postoperative atrial fibrillation in patients undergoing coronary artery bypass grafting (CABG) at different periods after acute myocardial infarction (AMI). It examines the efficacy of early administration of beta-adrenergic blocking agents (metoprolol) and amiodarone (in prophylactic doses) in the diminution of the risk of postoperative atrial fibrillation in different groups of patients. The article also discerns the effectiveness of digoxin in the management of episodes of postoperative atrial fibrillation.
Keywords: Coronary artery bypass grafting (CABG), prophylaxis, atrial fibrillation.
Introduction. Post-operative atrial fibrillation has been classified as the most spread kind of complication occurring in the earliest days after coronary artery bypass grafting (CABG). It is recorded in twenty to fifty percent of all patients in the early post-CABG period. Some rare cases of atrial fibrillation tend to resolve suddenly in a six-week period following the surgical intervention [1]. However, it augments four times the probability of stroke occurrence and three times the propensity for incidence of cardiogenic events capable to precipitate the death of hospitalized patients [2,5]. In addition, this kind of heart pace disturbance is often susceptible to impose a prolonged length of medical facility stay hence to considerably more expenditure in treatment and recovery after coronary artery bypass surgery [5].
Numerous clinical researches have demonstrated the effectiveness of amiodarone (class III antiarrhythmic drug) in the management of patients with atrial fibrillation. This drug has proven its ability to effectively maintain a physiologically normal rhythm in individuals with anomalies of cardiac muscles as well as in subjects presenting with cardiac conduction system defects [6,7,8]. As per suggestions of leading American institutions of cardiology, routine perioperative or early post-CABG beta-adrenergic receptor blocking by metoprolol is considered as standard treatment oriented to a compelling diminution of the risk of CABG-related atrial fibrillation.
Several studies have come to the conclusion that digoxin and nondihydrоpyridine calcium-channel blockers (verapаmil, diltiazеm) possess no consistent benefit for counteracting the occurrence of atrial fibrillation in the earliest days after open-chest heart surgery. However, they have proven their predominant roles in the management of this sort of heart rhythm disturbance in case it does already occur [3,4].
Purpose of the research. Analyze various strategies for prevention and management of atrial fibrillation in patients undergoing coronary artery bypass grafting surgery at various periods following acute myocardial infarction (AMI).
Materials and methods. This program comprised a total number of 105 individuals expected to undergo a scheduled CABG after an ST segment elevation and non-ST segment elevation myocardial infarction: 73 (69,52%) males plus 32 (30,48%) female. Their ages were between forty-one and seventy-two years old interval. The mean calculated value of their ages equaled 52.67±7.86 years.
The distribution of subjects in concordance with their age groups is illustrated below (tab.1)
Table 1 - Distribution of patients by age groups
| All subjects | 40 – 55 y.o. | 56-70 y.o. | 71 – 80 y.o. | |
| Male | 73 (69.52%) | 13 (12.38%) | 46 (43.8%) | 14 (13.33) |
| Females | 32 (30.48%) | 6 (5.71%) | 21 (20%) | 5 (4.71%) |
| All patients (both sexes) | 105 | 19 18.09% | 67 63.8% | 19 18.09% |
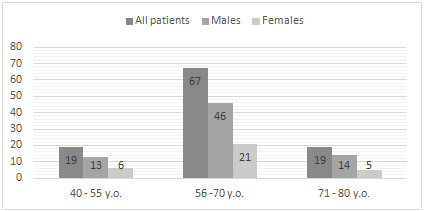
Fig. 1 - Distribution of subjects in concordance with their age and sex affiliations
Four groups of patients were formed relying upon the time allotment between the onset of acute myocardial infarction and the execution of coronary artery bypass grafting:
Group 1: CABG was executed in the first 10 days following AMI – 20 (19.04%) subjects: 13 males plus 7 females.
Group 2: CABG was executed in the time interval between the tenth and the thirtieth days that followed AMI– 20 (19.04%) subjects: 11 males plus 9 females.
Group 3: CABG was executed up to the fifth month following AMI – 23 (21.9%) subjects: 17 males and 6 females.
Group 4: The period of execution of CABG extended from the very beginning of the sixth month to the twelfth month following AMI– 42 (40%) subjects: 32 males, 10 females.
Strategy of medication administration.
The first branch of this strategy was mainly aimed at reducing the overall risk of intra-/ post-operative fibrillation of atria while the associated branch particularly focused on controlling ongoing episodes of atrial fibrillation. They were implemented as follow:
- Starting to prepare patients as early as possible by administering beta-adrenergic blocking agents (metoprolol: 100-150mg per day) beginning from the patient’s admission day and continuing the procedure up to the complete discharge of the patient from the healing facility.
- Few in-patients (in group 2 and group 4) presented with contraindications for beta-blocker administration. That led us to modify their treatment by replacing the agent by amiodarone dosed 600mg per os every day for about seven to ten days before the on-pump or off-pump manipulation on the heart with further correction of the dose (200mg per os and per day) until the discharge.
- In the postoperative period, digoxin and nondihydropyridine calcium-channel blockers (verapamil, diltiazem) were utilized in the composition of the management regimen with the purpose to arrest ongoing fibrillations but this experiment did not consider these two drugs as preventive medications.
Results and analytic discussion.
The obtained data showed that out of the 105 subjects under consideration, 14 (13.3%) subjects manifested atrial fibrillation during the early hours to days posterior to coronary artery bypass grafting. tab.2.
Table 2 - Classification of AF subsequent to CABG by groups
| Structure | Group №1 | Group №2 | Group №3 | Group №4 | |
| All subjects | 105 | 20 | 20 | 23 | 42 |
| Atrial fibrillation (number, percentage in each group) | 14(13.3%) | 5(25%)*^ | 5(25%)*^ | 3(13%)*# | 1(2.4%)^# |
The existing differences observed between groups №1 and №2 with groups №3 and №4 as well as between groups №3 and №4 are statistically reliable.
We calculated the duration of stay in the intensive care unit (ICU) of subjects under consideration and compared it to the stay prolongation of the subjects in the hospital in general. The outcomes are exposed below. Tab. 3.
Table 3 - Hospital stay profile
| Structure | Group №1 | Group №2 | Group №3 | Group №4 | |
| All subjects | 105 | 20 | 20 | 23 | 42 |
| Number of days spent in the ICU | 3.3±0,2 | 3.9±0.3 | 2.4±0.2* *P<0,05 | 3.1±0.2 | 3.7±0.4 |
| Duration of stay in the hospital (in days) | 23.5±2.1 | 21.75±2.0 | 28.05±1.4 | 23.2±2.2 | 22.3±1.3 |
The data stresses out that more cases of atrial fibrillation were recorded in the group №1 and group №2. Considering the fact that subjects of group №1 went through the operation in emergency, it is most likely that the preoperative prophylactic management with beta-blockers was not long enough in term of duration (number of days) in order to effectively diminish the postoperative risk of atrial fibrillation. Despite equal numbers of postoperative atrial fibrillation in both group №1 (CABG in the first 10 days following heart attack), and group №2 (CABG was performed in the interval between the 10th and the 30th days subsequent to AMI), the least medical facility stay was registered in group №2, which is statistically reliable.
Digoxin and calcium-channel blockers (verapamil, diltiazem) proved their effectiveness in controlling episodes of atrial fibrillation
Patients of group №3 and group №4 received beta-adrenergic blocking agents for an optimum period in the composition of their standard therapy of MI, which probably reduced the number of cases of atrial fibrillation in both of these mentioned groups.
Conclusion.
- Early administration of beta-blockers (metoprolol) and amiodarone in prophylactic doses results in the diminution of the risk of atrial fibrillation in patients after coronary artery bypass grafting operation.
- Digoxin can effectively control episodes of postoperative atrial fibrillation.
References
- Mariscalco G., Klersy C., Zanobini M. et al., “Atrial fibrillation after isolated coronary surgery affects late survival,” Circulation, vol. 118, no. 16, pp. 1612–1618, 2008.
- Roach G. W., Kanchuger M., Mangano C. M. et al., “Multicenter study of perioperative ischemia research group and the ischemia research and education foundation investigators. Adverse cerebral outcomes after coronary bypass surgery,” The New England Journal of Medicine, vol. 335, pp. 1857–1863, 1996.
- Rubin DA, Nieminski KE, Reed GE, Herman MV. Predictors, prevention, and long-term prognosis of atrial fibrillation after coronary artery bypass graft operations. J Thorac Cardiovasc Surg 1987;94:331-5.
- White HD, Antman EM, Glynn MA, et al. Efficacy and safety of timolol for prevention of supraventricular tachyarrhythmias after coronary artery bypass surgery. Circulation 1984;70:479-84.
- Aranki SF, Shaw DP, Adams DH, et al. Predictors of atrial fibrillation after coronary artery surgery: current trends and impact on hospital resources. Circulation 1996;94:390-7.
- Gold RL, Haffajee CI, Charos G, Sloan K, Baker S, Alpert JS. Amiodarone for refractory atrial fibrillation. Am J Cardiol 1986;57:124-7.
- Horowitz LN, Spielman SR, Greenspan AM, et al. Use of amiodarone in the treatment of persistent and paroxysmal atrial fibrillation resistant to quinidine therapy. J Am Coll Cardiol 1985;6:1402-7.
- Nicklas JM, McKenna WJ, Stewart RA, et al. Prospective, doubleblind, placebo-controlled trial of low-dose amiodarone in patients with severe heart failure and asymptomatic frequent ventricular ectopy. Am Heart J 1991;122:1016-21.