ЭПИДЕМИОЛОГИЧЕСКИЕ АСПЕКТЫ ПОСТ КАРДИОХИРУРГИЧЕСКИХ ГНОЙНО-СЕПТИЧЕСКИХ ИНФЕКЦИЙ В ЗАВИСИМОСТИ ОТ ОСНОВНОГО ДИАГНОЗА
ЭПИДЕМИОЛОГИЧЕСКИЕ АСПЕКТЫ ПОСТ КАРДИОХИРУРГИЧЕСКИХ ГНОЙНО-СЕПТИЧЕСКИХ ИНФЕКЦИЙ В ЗАВИСИМОСТИ ОТ ОСНОВНОГО ДИАГНОЗА
Научная статья
ORCID: 0000-0002-3992-9242,
Государственный университет медицины и фармации им. Н.Тестемицану, Кишинёв, Молдова
* Корреспондирующий автор (aliona.nastas[at]usmf.md)
АннотацияВ течение последнего десятилетия, инфекции связанные с оказанием медицинской помощи (ИСМП), становится все более тревожной проблемой общественного здравоохранения даже в развитых и промышленно развитых странах. Эти инфекции имеют специфические эпидемиологические аспекты в разных профильных стационарах. Исследования демонстрирует приобретение гнойно-септических пост-кардиохирургических инфекций в профильном стационаре в зависимости от основного диагноза. Было доказано, что частота гнойно-септических пост-кардиохирургических инфекций выше у пациентов, оперированных в срочном порядке, большинство гнойно-септических инфекций регистрируются у пациентов, проходящих шунтирование, шунтирование плюс одно протезирование плюс одна пластика, шунтирование плюс одно протезирование плюс две пластики, шунтирование плюс одна пластика, шунтирование плюс два протезирования плюс одна пластика, с основными диагнозами: ишемическая болезнь сердца, дискантная аневризма (синдром Марфана), аортальный/ митральный / трехстворчатый порок, эндокардит, ишемическая кардиопатия.
Ключевые слова: гнойно-септические инфекции, эпидемиологический надзор, эпидемический процесс, факторы риска, сердечные заболевания.
EPIDEMIOLOGICAL ASPECTS OF POST-CARDIOSURGICAL SEPTIC-PURULENT INFECTIONS BASED ON BASIC DIAGNOSIS
Research article
Nastas A.T. *
ORCID: 0000-0002-3992-9242,
N.Testemitanu State University of Medicine and Pharmacy, Chisinau, Moldova
* Corresponding author (aliona.nastas[at]usmf.md)
AbstractOver the last decade, healthcare associated infections (HAI) have been increasingly alarming as a public health problem even in developed and industrialized countries. These infections have a specific epidemiological aspect in hospitals with different medical profiles. This study demonstrates the acquisition of septic-purulent nosocomial infections in the hospital with cardiosurgical profile depending on the basic diagnosis. It has been shown that the incidence of post-cardiosurgical septic-purulent infections is higher in emergency patients, most post-cardiosurgical septic-purulent infections are recorded in patients undergoing bypass, bypass plus one prosthesis plus one plasty, bypass plus one prosthesis plus two plasties, bypass plus one plasty, bypass plus two prostheses plus one plasty, having the diagnosis of cardiopathy, dissecting aneurism (Marfan syndrome), defect of aortic / mitral/ tricuspid valve, endocarditis, cardiopathy.
Keywords: septic-purulent infections, epidemiological surveillance, epidemic process, risk factors, cardiac diseases.
IntroductionHealthcare associated infections (HAI) are a public health problem even in developed and industrialized countries. Of the 10% of the European population hospitalized each year, 5% of them (3.8% - general departments, 15.3% - in the intensive care units (ICU) departments) acquire at least one nosocomial infection. One million seven hundred fifty thousand hospitalized patients are affected annually in Europe through HAI, the mortality rate reaches 175,000 deaths each year [1].
Studies in the USA indicate that nosocomial infections amount to approximately two million, with deaths of 90,000 per year [2]. Health associated infections are complications due to hospitalization and lead to increased morbidity and mortality [3], [4], [5]. These infections prolong hospitalization, require much more extensive diagnosis and treatment, and are associated with additional costs [5], [6], [7]. Numerous published studies describe the risk factors in surgical site infection, especially for sternal infection / deep wound infection. A meta-analysis by a number of Italian researchers to improve the management of infections in cardiac surgery units has highlighted a number of risk factors associated with deep wound infections and surgical risk factors (surgery, duration of operation, emergency mode [8], [9], [10].
The full economic impact due to the morbidity through post-cardiosurgical septic-purulent infections in the period of study 2010 - 2013 in the Republic of Moldova totals MDL 53,111,959.61. Costs incurred as a result of septic-purulent nosocomial cardio-surgical infections have a negative impact, requiring urgent prophylaxis, changing the surveillance and control system of these infections to optimize expenditure and reduce the negative impact on public health [11].
Risk factors for patients with wound infection associated with cardiac surgery were the urgent surgery (18.1%) and the surgical method (procedure), which included operation on the valve defect (14.7%), coronary surgery (65.8%), combined surgery (14.1%), other heart surgery (5.4%) [12]. In the Republic of Moldova epidemiological studies on morbidity through post-cardiosurgical septic-purulent infections based on basic diagnosis have not been performed.
Material and methods
The study was conducted at the Republican Clinical Hospital "Timofei Mosneaga" during the period of 2010-2013, it includes the active identification of the septic-purulent infections through the research of 1332 records of the hospitalized patients in the Cardiac Surgery of Acquired Defects Department. The recommended case definitions for nosocomial infections with criteria for each location are those set out in the Nosocomial Infection Guidelines, edition II, 2009 [13], and the Guidelines for Surveillance, Prevention and Control of Nosocomial Infections in SCJUPBT in 2016 [14]. The frequency indexes of cardiovascular septic-purulent infections morbidity in 1,000 patients hospitalized or treated.
Results
Of the 418 cases with septic-purulent infections actively detected by the examination of the patient records during the years 2010 - 2013 in the Department of Cardiac Surgery of Acquired Defects, 403 patients or 96.41% were scheduled for surgery, 15 or 3.59% were operated on urgent basis (Table 1, Figure 1).
Table 1 – Incidence of post-cardiosurgical septic-purulent infections based on the type of the surgery during the years 2010 - 2013
| Years | Scheduled | Urgent | ||||||
| Total no. of operated patients | abs | % | By 1000 surgeries | Total no. of operated patients | abs | % | By 1000 surgeries | |
| 2010 | 338 | 120 | 94.49 | 355.03 | 15 | 7 | 5.51 | 466.67 |
| 2011 | 256 | 96 | 97.96 | 375.00 | 4 | 2 | 2.04 | 500.00 |
| 2012 | 246 | 91 | 96.81 | 369.92 | 3 | 3 | 3.19 | 1000.00 |
| 2013 | 321 | 96 | 96.97 | 299.07 | 6 | 3 | 3.03 | 500.00 |
| Total | 1161 | 403 | 96.41 | 347.11 | 28 | 15 | 3.59 | 535.71 |
During the years 2010 – 2013, observing each year, the majority of patients from 94.49% in 2010 up to 96.97% in 2013 were scheduled for surgery and urgent surgeries were performed on 2.04% in 2011 up to 5.51% in 2010.
Fig. 1 – Distribution of post-cardiosurgical cases of septic-purulent infections based on surgery type during the years 2010 – 2013 (%)
The septic-purulent infections incidence is higher in patients who are operated urgently (535.71‰) compared to those operated on a scheduled basis (347.11‰) (Figure 2). During the years 2010 - 2013, the septic-purulent infections incidence is also the highest in emergency patients: in 2010 it was 1.32 times higher, in 2011 by 1.34 times, in 2012 by 2.71 times, in 2013 by 1.68 times compared to scheduled operated patients.
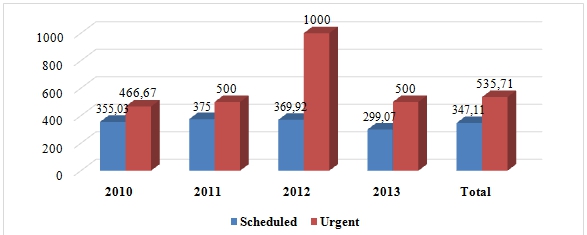
Fig. 2 – Incidence of post-cardiosurgical septic-purulent infections based on type of the surgery (‰)
Of the total of 418 cases of cardio-surgical septic-purulent infections during the years 2010-2013, 135 or 32.3% are wound infections, 95 or 22.73% are association related infections, 79 or 18.9% are nosocomial respiratory infections, 71 cases or 16,99% are cardiovascular infections, 20 cases or 4,78% are bone and joint infections (Figure 3).
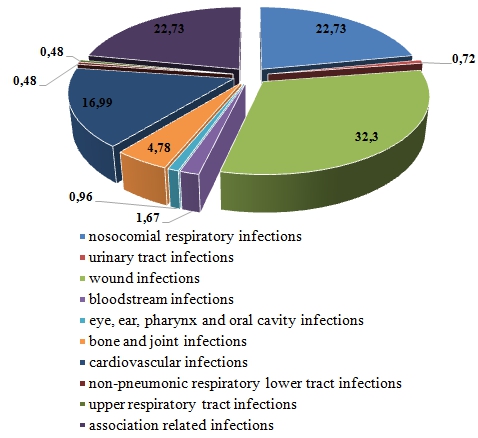
Fig. 3 – Structure of post-cardiosurgical septic-purulent infections during the years 2010 – 2013 (%)
Other cases from 0.48% to 1.67% are infections of the urinary tract (0.72%), bloodstream infections (1,67%), eye, ear, pharynx and oral cavity infections (0,96%), non-pneumonic lower respiratory tract infections (0,48%) and upper respiratory tract infections (0,48%).
They were 95 cases (22.73%) of septic-purulent infections reported in patients who underwent one bypass, 55 cases (13.16%) suffered bypass plus one prosthesis plus one plasty, 52 cases (12.44%) - bypass plus one prosthesis plus two plasties, 37 or 8.85% - bypass plus one plasty, 36 or 8.61% - bypass plus two prostheses plus one plasty, 26 or 6.22% - bypass plus two plasties (Figure 4).
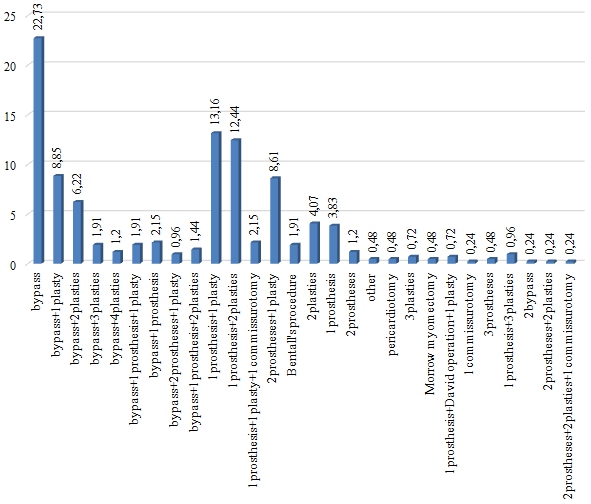
Fig. 4 – Structure of the post-cardiosurgical septic-purulent infections morbidity based on surgeries performed, years 2010 – 2013 (%)
Other cardiac surgeries that are performed consist of 0.24 - 4.07% of post-cardiosurgical septic-purulent infections.
Of 418 cases with septic-purulent infections actively detected during the years 2010 - 2013, 254 or 60.77% of patients had a basic diagnosis of cardiopathy, 106 or 25.36% patients - valvulopathy, 22 or 5.26% of patients - endocarditis, 11 or 2.83% of patients – defect of aortic/mitral/tricuspid valve, 10 patients or 2.39% rheumatism, 8 patients or 1.91% - dissecting aneurism (Marfan syndrome), 4 or 0.96% myxoma, 1 patient or 0.24% - pericarditis, 2 or 0.48% patients - other diagnoses (Figure 5).
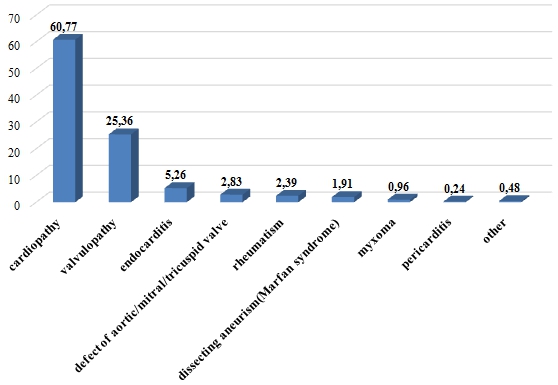
Fig. 5 – Distribution of post-cardiosurgical septic-purulent infections based on basic diagnosis during the years 2010 – 2013 (%)
Throughout the period of the study, patients with cardiopathy and valvulopathy were found to be 79 - 88% in different years.
Another situation occurs when calculating the incidence through septic-purulent infections based on basic diagnosis. The highest incidence, 533.33 per 1000 operated patients is highlighted in patients with dissecting aneurism (Marfan syndrome), followed by defect of aortic/mitral/tricuspid valve with 500.0‰, then other diagnoses - 400.0‰, endocarditis - 392.86‰, cardiopathy - 391.98‰, valvulopathy - 279.68‰, myxoma - 266.67‰, rheumatism - 227.27‰ and pericarditis – 200.0‰ (Figure 6).
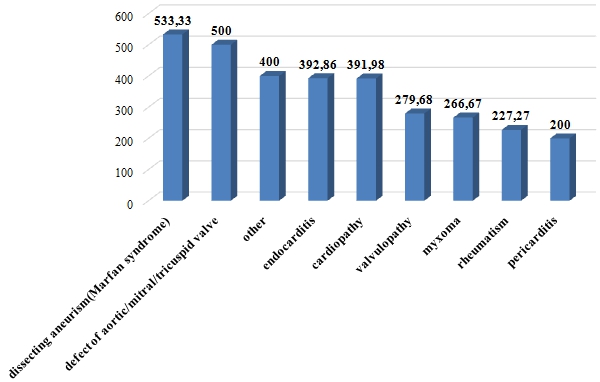
Fig. 6 – Incidence of post-cardiosurgical septic-purulent infections based on basic diagnosis (‰)
In 2010, the highest incidence of septic-purulent infections based on basic diagnosis was 449.1‰ in patients with cardiopathy, followed by patients with dissecting aneurism (Marfan syndrome) - 400.0‰, those with defect of aortic/mitral/tricuspid valve - and endocarditis with 333.33%. This year, no septic-purulent infections was recorded in patients with pericarditis and other diagnoses.
In 2011, the highest incidence of septic-purulent infections based on basic diagnosis was recorded in patients with cardiopathy, accounting for 561.22‰, followed by patients with myxoma - 500.0‰ and patients with endocarditis - 333.33‰. This year, no cases were recorded in patients with pericarditis and dissecting aneurism (Marfan syndrome).
The highest incidence of septic-purulent infections in 2012 was in patients with other diagnoses - 1000.0 per 1000 operated patients, followed by patients with dissecting aneurism (Marfan syndrome) - 750.0‰, defect of aortic/mitral/tricuspid valve - 666, 67‰ and endocarditis - 571.43‰. This year, the lowest incidence occurred in patients with rheumatism - 125.0‰.
In 2013, patients with the basic diagnosis of defect of aortic/mitral/tricuspid valve - had the highest incidence of 1000‰, followed by patients with dissecting aneurism (Marfan syndrome) with 600.0‰, pericarditis - 500.0‰. This year, no SPNI was recorded in patients with myxoma and those with other diagnoses.
Discussion
The study conducted in the cardiac surgery profile demonstrates the increased incidence of morbidity through septic-purulent infections in emergency patients - which is 535.71‰ compared to those who are operated on a scheduled basis with the incidence of 347.11‰. Of the total of septic-purulent infections 32.3% are surgical wound infections, 22.73% are association related infections, 18.9% are nosocomial respiratory infections, 16.99% are cardiovascular infections, 4.78% are bone and joint infections. The riskiest basic diagnoses for the acquisition of post-cardiosurgical septic-purulent infections are: 449.1‰ cardiopathy, followed by patients with dissecting aneurism (Marfan syndrome) - 400.0‰, those with defect of aortic/mitral/tricuspid valve and endocarditis with 333,33‰, and the riskiest cardiac surgeries are: 22.73% in patients who underwent one bypass, 13.16% supported bypass plus one prosthesis plus one plasty, 12.44% - bypass plus one prosthesis plus two plasties, 85% - bypass plus one plasty, 8.61% - bypass plus two prostheses plus one plasty, 6.22% - bypass plus two plasties. The findings can help to improve the system of prophylaxis of post-cardiosurgical septic-purulent infections.
Conclusion
- The incidence of post-cardiosurgical septic-purulent infections is higher in patients that underwent urgent surgeries than those patients who were operated on a scheduled basis.
- Most post-cardiosurgical septic-purulent infections are recorded in patients who underwent one bypass, bypass plus one prosthesis plus one plasty, bypass plus one prosthesis plus two plasties, bypass plus one plasty, bypass plus two prostheses plus one plasty.
- The highest incidence of post-cardiosurgical septic-purulent infections occurs in patients diagnosed with dissecting aneurism (Marfan syndrome), defect aortic/mitral/tricuspid valve, endocarditis, cardiopathy.
| Конфликт интересов Не указан. | Conflict of Interest None declared. |
Список литературы / References
- Report of the European Science Foundation [Электронный ресурс] 2005 URL: http://www.escmid.org/ (дата обращения:19.03.2019)
- Esker D.J. Investments in high payoff technologies could reduce toll of infections / Esker DJ, Carroll KC. // ASM News. 2005; 71 (12): 576-581
- Geffers C. Mortality attributable to hospital-acquired infections among surgical patients. Infect Control Hosp Epidemiol / Geffers C. 2008; 29: 1167-1170
- Aranaz-Andres J.M. Incidence of adverse events related to health care in Spain: results of the Spanish National Study of Adverse Events / Aranaz-Andres J.M. J Epidemiol Community Health.2008; 62: 1022-1029
- Geffers K. Nosocomial infections and multidrug- resistant organisms in Germany / Geffers K. Gastmayyer P. Dtsch Arztebl Int. 2011 Fev; 108 (6): 87-93
- Pittet D. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality / Pittet D. Dzham. 1994; 271: 1598-1601
- Beyersmann J. Use of multistate models to assess prolongation of intensive care unit stay due to nosocomial infection / Beyersmann J. Infect Control Hosp Epidemiol. 2006; 27: 493-499
- Buya A. An update review on risk factors and scales for prediction of deep sternal wound infections / Buya A. Int Wound J. 2012; avgust; 9 (4): 372 -86
- Попов Д.А. Послеоперационные инфекционные осложнения в кардиохирургии: частота развития, факторы риска, этиология, особенности патогенеза, оптимизация диагностики / Попов Д.А. №5, 2011. С.10-14 журнал Анналы хирургий. Москва
- Миролюбова О.А. Биопротезирование клапанов сердца / Миролюбова О. А., Мизинцева М. А. №4S1(132), 2016, с.58. Журнал Российский кардиологический журнал. Москва
- Nastas A.T. The socio-economic impact of post cardiac surgery patients with septic-purulent nosocomial infections / Nastas A.T. // International Research Journal № 11 (77) Part 1, 2018, P. 166-172, DOI: https://doi.org/10.23670/IRJ.2018.77.11.032
- Jolivet S. Surgical site infection with extended-spectrum b-lactamase producing Enterobacteriaceae after cardiac surgery: incidence and risk factors Clinical Microbiology and Infection / Jolivet S. 24 (2018) 283-288
- Nosocomial Infection Guidelines, edition II, 2009, Kishinev
- Guidelines for Surveillance, Prevention and Control of Nosocomial Infections (CPCIN) in SCJUPBT) 2016 .
Список литературы на английском языке / References in English
- Otchet Yevropeyskogo nauchnogo fonda za 2005 g [Report of the European Science Foundation] [Electronic resource] 2005. URL: http://www.escmid.org/ (accessed:03.2019)
- Esker D.J. Investitsii v tekhnologii s vysokoy otdachey mogut sokratit' chislo infektsiy [Investments in high payoff technologies could reduce toll of infections] / Esker DJ, Carroll KC. // ASM News. 2005; 71(12): 576-581
- Geffers C., et al., , Obuslovlennaya vnutribol'nichnymi infektsiyami sredi khirurgicheskikh patsiyentov. Infekt Kontrol' Gospital' Epidemiol [Mortality attributable to hospital-acquired infections among surgical patients. Infect Control Hosp Epidemiol]. 2008; 29:1167-1170
- Aranaz-Andres J.M. Chastota nezhelatel'nykh yavleniy, svyazannykh so zdravookhraneniyem v Ispanii: rezul'taty ispanskogo natsional'nogo issledovaniya pobochnykh yavleniy [Incidence of adverse events related to health care in Spain: results of the Spanish National Study of Adverse Events] / Aranaz-Andres J.M. J Epidemiol Community Health. 2008;62:1022-1029
- Geffers C. Nozokomial'nyye infektsii i organizmy s mnozhestvennoy lekarstvennoy ustoychivost'yu v Germanii [Nosocomial infections and multidrug- resistant organisms in Germany] / Geffers C., Gastmeier P. Dtsch Arztebl Int. 2011 Feb;108(6):87-93
- Pittet D. Nozokomial'naya infektsiya krovotoka u kriticheski bol'nykh patsiyentov. Chrezmernaya prodolzhitel'nost' prebyvaniya, dopolnitel'nyye raskhody i svyazannaya s etim smertnost [Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality] / Pittet D. Jama. 1994; 271:1598-1601
- Beyersmann J. Ispol'zovaniye mnogogosudarstvennykh modeley dlya otsenki prodleniya prebyvaniya otdeleniya intensivnoy terapii v svyazi s vnutribol'nichnoy infektsiyey. Infect Control Hosp Epidemiol [Use of multistate models to assess prolongation of intensive care unit stay due to nosocomial infection. Infect Control Hosp Epidemiol] / Beyersmann J. 2006; 27:493-499
- Buja A. Obnovlennyy obzor faktorov riska i shkal dlya prognozirovaniya glubokikh infektsiy rany grudiny [An update review on risk factors and scales for prediction of deep sternal wound infections] / Buja A. Int Wound J. 2012; Aug; 9(4): 372 -86
- Popov D.A. Posleoperacionnye infekcionnye oslozhneniya v kardiohirurgii: chastota razvitiya, faktory riska, etiologiya, osobennosti patogeneza, optimizaciya diagnostiki [Postoperative infectious complications in cardiac surgery: the incidence of development, risk factors, etiology, pathogenesis features, optimization of diagnosis] / Popov D.A. "No. 5, 2011. Pages 10-14, Annaly hirurgij [Annals of Surgery]. Moscow [in Russian]
- Mirolyubova O. A.Bioprotezirovanie klapanov serdca [Heart Valve Bioprosthetics] / Mirolyubova O. A., Mizintseva M. A. // Zhurnal "Rossijskij kardiologicheskij zhurnal [Journal of the Russian Cardiology Journal]. Moscow, 4S1 (132), 2016, p.58. [in Russian]
- Nastas A.T. Sotsial'no-ekonomicheskoye vliyaniye patsiyentov posle kardiokhirurgicheskikh operatsiy na gnoyno-septicheskuyu infektsiyu, Mezhdunarodnyy nauchno-issledovatel'skiy zhurnal [The socio-economic impact of post cardiac surgery patients with septic-purulent nosocomial infections] / Nastas A.T. // International Research Journal № 11 (77) Vol. 1 November 2018, стр. 166-172, DOI: https://doi.org/10.23670/IRJ.2018.77.11.032
- Jolivet S. Infektsiya v meste operatsii s pomoshch'yu b-laktamazy, produtsiruyushchey enterobakterii rasshirennogo spektra, posle operatsii na serdtse: chastota i faktory riska Klinicheskaya mikrobiologiya i infektsiya [Surgical site infection with extended-spectrum b-lactamase producing Enterobacteriaceae after cardiac surgery: incidence and risk factors Clinical Microbiology and Infection] / Jolivet S. 24 (2018) 283-288
- Rukovodstvo po vnutribol'nichnoy infektsii, edition II [Nosocomial Infection Guidelines, edition II], 2009, Chisinau
- Rukovodstvo po nadzoru, profilaktike i kontrolyu nozokomial'nykh infektsiy v SKYUPBT [Guidelines for Surveillance, Prevention and Control of Nosocomial Infections (CPCIN) in SCJUPBT] ("Pius Brinzeu" Emergency Clinical Hospital Timisoara) in 2016