ВЗАИМОСВЯЗЬ ФАКТОРА РОСТА ФИБРОБЛАСТОВ-23 (FGF-23), sKLOTHO, ТРОПОНИНА-I У БОЛЬНЫХ ХРОНИЧЕСКОЙ БОЛЕЗНЬЮ ПОЧЕК
Милованова Л.Ю.1, Козловская Л.В.2, Милованова С.Ю.3, Киякбаев Г.Г.4 Милованов Ю.С.5,Таранова М.В.6, Фомин В.В.7, Мухин Н.А.8, Рогова И.В.9, Андросова Т.В.10, Бровко М.Ю.11, Дударева А.В.12, Деревягина О.С.13
1ORCID: 0000-0002-5599-0350, Кандидат медицинских наук, доцент кафедры, 2Доктор медицинских наук, профессор, 3ORCID: 0000-0002-2687-6161, Доктор медицинских наук, ведущий научный сотрудник, 4Кандидат медицинских наук, ассистент кафедры, 5ORCID: 0000-0001-7450-2861, Доктор медицинских наук, профессор, 6Кандидат медицинских наук, ассистент кафедры, 7Доктор медицинских наук, профессор, 8Доктор медицинских наук, профессор, академик РАН, 9Кандидат медицинских наук, 10Кандидат медицинских наук, ассистент кафедры, 11Аспирант,12Интерн, 13Ординатор, Первый Московский Государственный Медицинский Университет им. И.М.Сеченова, Кафедра внутренних, профессиональных болезней и пульмонологии, Кафедра нефрологии и гемодиализа, Клиника нефрологии, внутренних и профессиональных болезней
Работа выполнена при поддержке Российского Научного Фонда (грант N 1415-00947 2014 г.)
ВЗАИМОСВЯЗЬ ФАКТОРА РОСТА ФИБРОБЛАСТОВ-23 (FGF-23), sKLOTHO, ТРОПОНИНА-I У БОЛЬНЫХ ХРОНИЧЕСКОЙ БОЛЕЗНЬЮ ПОЧЕК
Аннотация
Введение и цель исследования: Повышение уровня фактора роста фибробластов (FGF-23) в сыворотке крови больных хронической болезнью почек (ХБП) вносит вклад в ремоделирование сердца и сосудов. Точные механизмы, с помощью которых FGF-23 может приводить к повреждению миокарда, пока не установлены. Полагают, что эффекты FGF-23 на сердце могут быть обусловлены нарастающим дефицитом белка Klotho по мере прогрессирования ХБП. Умеренно повышенные уровни тропонинов характерны для пациентов с ХБП даже при отсутствии у них клинических проявлений кардиоваскулярных осложнений. Целью исследования являлось определить наличие взаимосвязи между FGF-23, Klotho и тропонином-I в сыворотке крови у больных ХБП.
Материалы и методы: Сывороточные уровни FGF-23(Human FGF-23 ELISA kit with antibodies to full FGF-23 molecule), Klotho (Human soluble Klotho with antiKlotho monoclonal antibodies), Тропонина-I (high-sensitive assay ) были исследованы у 110 пациентов с ХБП 1-5D стадиями. Инструментальные методы обследования включали: электрокардиографию (ЭКГ), эхокардиографию (ЭХО-КГ - ИММЛЖ, степень кальцификации сердца (КС), оцененную с помощью полуколичественной балльной шкалы), сфигмаграфию ( индексы аугментации(жесткости) сосудов (ИА), скорость пульсовой волны(СПВ), центральное(аортальное) артериальное давление (ЦАД), кровоснабжение субэндокарда (КСЭ) – с помощью прибора «Сфигмакор»(Австралия). Исследование одобрено локальным этическим комитетом.
Результаты: Динамика сывороточных уровней FGF-23, Klotho и тропонина-I изменялась в зависимости от стадии ХБП. Мы выявили следующие корреляции: FGF-23 с тропонином-I [r= 0,521; p<0,01], ИА [r=0,598; p<0,01], КС[r = 0,498; p <0,05], ИММЛЖ [r= 0,628; p<0,01], концентрическим типом ремоделирования миокарда (РМ) [r=0,598; p<0,01], диастолической дисфункцией левого желудочка сердца (ДД) [r= 0,479; p<0,01], КСЭ [r= - 0,449;p<0,01]. У пациентов, имеющих повышенный уровень ЦАД ( >120/ 80 мм. рт. ст.), и у пациентов с нормальным уровнем ЦАД (90-120/60-79 мм. рт. ст.) средние уровни FGF-23 в сыворотке крови были примерно одинаковыми [629+118 and 489+85],что может свидетельствовать о независимом от уровня ЦАД влиянии FGF-23 на миокард. В то же время сывороточный уровень тропонина-I коррелировал с ИММЛЖ [r = 0,544; p<0,01], концентрическим типом РМ [r=0,449;p<0,01], КСЭ [r= - 0,514;p<0,01], ДД [r= 0,492; p<0,01], длительностью заболевания почек [r = 0,468; p <0,05], наличием аритмий, по данным ЭКГ [r=0,445;p<0,05], уровнем ЦАД [r=0,534;p<0,01]. Между сывороточными уровнями Klotho и: тропонина-I [r= - 0,537; p<0,01], СПВ [r=-0,647;p<0,01], степенью КС [r=- 0,612; p<0,01], ИММЛЖ [r = - 0,539; p <0,01], концентрическим типом РМ [r=- 0,528;p<0,01] мы выявили отрицательную взаимосвязь. По данным многофакторного анализа, отмечено наличие ассоциации между повышенным уровнем тропонина-I и: пониженным уровнем Klotho, повышенным уровнем FGF-23, повышенным уровнем ЦАД у больных ХБП, включенных в исследование.
Заключение: По нашим данным, умеренно повышенный уровень тропонина-I в сыворотке крови ассоциирован с повышенным сывороточным уровнем FGF-23 и с низким Klotho, у пациентов с ХБП с 1-5D стадиями без клинических признаков кардиоваскулярных осложнений.
Ключевые слова: хроническая болезнь почек, FGF-23, Klotho, тропонин-I.
Milovanova L.Y.1, Kozlovskaya L.V.2, Milovanova S.Y.3, Kiyakbaev G.G.4, Milovanov Y.S.5, Taranova M.V.6, Fomin V.V.7, Mukhin N.A.8, Rogova I.V. 9, Androsova T.V.10, Brovko M.Y.11, Dudareva A.V.12, Dereviygina O.S.13
1MD, Associate professor, 2Professor, MD, 3MD,4MD, 5Professor, MD, 6MD, 7Professor, MD, 8Professor, MD, 9MD, 10MD, 11Postgraduate student, 12Postgraduate student, 13Postgraduate student, I.M. Sechenov First Moscow State Medical University, Department of internal, occupational diseases and pulmonology, Department of nephrology and hemodialysis, Hospital of nephrology, internal and occupational disease
The work was supported by the Russian Science Foundation (grant No 14-15-00947 2014 year)
ASSOCIATIONS OF FIBROBLAST GROWTH FACTOR 23, SOLUBLE KLOTHO, TROPONIN I IN CKD PATIENTS
Abstract
INTRODUCTION AND AIMS: Increased levels of fibroblast growth factor 23 in serum (sFGF-23) throw in cardiac remodeling in сronic kidney disease (CKD) patients. The exact mechanisms by which sFGF-23 damages myocardium have been not determined yet. It is believed the effects of sFGF-23 to the heart may be caused by Klotho deficiency (sKlotho) in CKD. The some elevated levels of troponins are common among CKD patients, even if they don’t have a symptomatic cardiovascular disease (sCVD). The study goal was to examine the connections between sFGF-23, sKlotho, Troponin-I (Tr-I) in CKD patients.
METHODS: sFGF-23 (Human FGF-23 ELISA kit with antibodies to full FGF-23 molecule), sKlotho (Human soluble Klotho with antiKlotho monoclonal antibodies), Tr-I (high-sensitive assay ), calcium, phosphorus, parathyroid hormone were measured in 110 patients with CKD stages 1-5, taking from outpatients department of First Moscow State Medical University, Russia. Instrumental methods of examination included: an electrocardiogram (ECG), echocardiogram ( LVMI, the degree of heart calcification (DHC), assessed by semiquantitative scale), sphygmagraphy (augmentation indexes (AI), pulse wave velocity (PWV), central (aortic) arterial blood pressure (CBP) and blood supply of endocardium (BSE) with a device "Sphigmakor" (Australia). The study was approved by the local ethical committee. All procedures were performed in accordance with Helsinki Declaration.
RESULTS: Assessment of sKlotho, sFGF-23 and Tr-I resulted in its changed as CKD progression. We found correlations of sFGF-23 with Tr-I [r= 0,521; p<0,01], AI [r=0,598; p<0,01], DHC [r = 0,498; p <0,05], LVMI [r= 0,628; p<0,01], the concentric myocardial remodeling (CMR) [r=0,598; p<0,01], diastolic dysfunction of the left ventricle (DDLV) [r= 0,479; p<0,01], BSE [r= - 0,449;p<0,01]. In the patients with increased CBP (> 120/80 mm. Hg) and in normal CBP (90-120 / 60-79mm. Hg) mean levels of sFGF-23 were about the same [629+118 and 489+85], indicating about an independent from the CBP action of FGF-23 on the myocardium. In the same time serum Tr-I correlated with LVMI [r = 0,544; p<0,01], CMR [r=0,449;p<0,01], BSE [r= - 0,514;p<0,01], DDLV [r= 0,492; p<0,01], kidney disease duration in months [r = 0,468; p <0,05], presence of arrhythmias in ECG [r=0,445;p<0,05], CBP levels [r=0,534;p<0,01]. Between sKlotho and Tr-I [r= - 0,537; p<0,01], PVW [r=-0,647;p<0,01], DHC [r=- 0,612; p<0,01], LVMI [r = - 0,539; p <0,01], CMR [r=- 0,528;p<0,01] we found negative relations. Multivariate analyses showed association of some elevated Tr-I serum levels with decreased of sKlotho, increased of sFGF-23 and increased of CBP in CKD.
CONCLUSIONS: In our study some elevated Tr-I levels was associated with increased sFGF-23 connected with Klotho deficiency in CKD patients without sCVD. sFGF-23-associated CMR may throw in elevated Tr-I levels observed in CKD.
Keywords: chronic kidney disease (CKD), FGF-23, sKlotho, troponins. The results of epidemiological studies allow to consider chronic kidney disease (CKD) as an independent predictor of appearance and progression of cardiovascular complication (CC), the risk of which in patients with renal insufficiency, including the young persons, increasing to 100 times and more [1,2].Despite of advances in the management of patients with CKD, including those treated by hemodialysis (HD), the frequency of CC is still one of the leading causes of death in these patients [3]. It becomes clearer that despite the high prevalence of traditional risk factors such as diabetes, arterial hypertension, atherosclerosis and others in CKD population but only their influence it can not be explained such a high mortality in patients with CKD. Understanding of CC pathogenesis in CKD is necessary to develop new therapeutic strategies to reduce risk of death in this cohort.
Currently, a most important role in CC genesis is given to serum FGF-23 (sFGF-23) and Klotho (sKlotho) [4]. sFGF- 23, produced by osteocytes, its main biological role - regulation of phosphorus, vitamin D, PTH metabolism. It was later shown an elevated sFGF-23 is associated with a high risk of death from CC and considered now as an early marker of uremic CC [5, 6]. However, the exact ways of sFGF-23 action have been not determined yet. It is believed the effects of sFGF-23 to the heart may be caused by its non-selective binding to FGF-1-receptors in the heart because of significant increase of sFGF-23 in the Klotho deficiency situation as CKD progression [7].
Klotho protein was named in honor of one from the goddesses of Greek mythology- Klotho, spinning the thread of human life, and therefore was identified as a «protein of a youth», « life protein» [8 9].
In the human body Klotho is produced by proximal tubule cells and exists in two forms - the transmembrane (tmKlotho) and extracellular (secreted) form (sKlotho). In Makoto K. study it was found that the tmKlotho is a co-receptor for sFGF-23 and is involved in the regulation of metabolism of phosphorus, calcium and vitamin D. sKlotho is secreted into the bloodstream and functions as an endocrine factor [8, 9].
The experiment revealed that damage of Klotho gene in mice causes multicomponent syndrome including premature aging, hyperphosphatemia, hypercalcaemia and hypervitaminosis D. [9]
To date, according to the literature [8,10,11], it is known that the reduction in sKlotho levels in patients with CKD is accompanied by loss of renal function, aggravation of hypertension, causes ectopic calcification, remodeling of the heart and blood vessels.
On the other hand, it was shown that sKlotho in healthy people can act as a humoral factor: high expression of sKlotho in lesions of kidney function in experiment is provided cardiovascular protection. [9,10,12].
Despite that the role of sFGF-23 and sKlotho has been studied extensively in patients with CKD there are many controversial issues concerning the relationship between these biomarkers at various stages of CKD and the specific mechanisms of their effects on the cardiovascular system.
It was found also patients with CKD often marked increase in troponins even in the absence of symptomatic CC[13]. Given the impact of sFGF-23 and sKlotho in the CC, we conduct a cross-section study to test the hypothesis are there associations between of sFGF-23, sKlotho and troponin I (Tr-I) in CKD patients?
Materials and Methods: 110 patients with CKD stages 1-5D without symptomatic CC (65 men and 66 women, aged 20-75 years, mean age at enrollment 41 ± 6,7 years) were recruited from outpatient nephrology department at the First Moscow State Medical University in Russia. sFGF-23 (Human FGF-23 ELISA kit using antibodies to full FGF-23 molecule), sKlotho (Human soluble Klotho with antiKlotho monoclonal antibodies), Tr-I (high-sensitive assay) were measured in all study patients in addition to routine tests. Instrumental methods of examination included: an electrocardiogram (ECG), echocardiogram ( left ventricular mass index – LVMI, injection fraction, degree of heart calcification (DHC) assessed by semiguantitative scale), «Sphygmacor» ( pulls wave velocity (PWV), augmentation (stiffness) indexes (AI), blood supply of endocardium (BSE), central (aortal) (CBP) and brachial arterial pressure. The study was approved by the Institutional Review Boards of the FMSMU. All procedures were performed in accordance with Helsinki Declaration.Results: Assessment of sFGF-23, sKlotho and Tr-I levels resulted in its changed in CKD progression (fig.1,2).
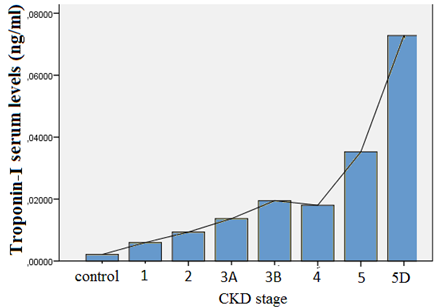
Fig. 1 - The relationship between Tr-I and CKD stage
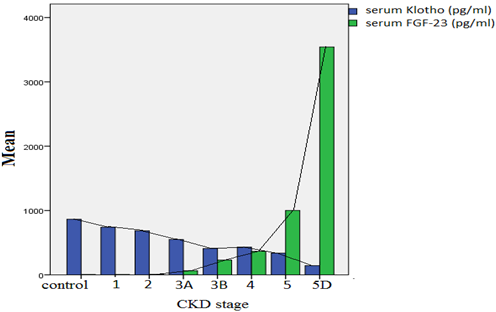
Fig. 2 - The relationship between sFGF-23, sKlotho and CKD stage
We found also correlations of sFGF-23 with Tr-I [r= 0,521; p<0,01] levels (Fig.3), PVW [r=0,514;p<0,01], DHC [r = 0,498; p <0,05], LVMI [r= 0,628; p<0,01], CMR) [r=0,598; p<0,01], DDLV [r= 0,479; p<0,01], BSE [r= - 0,449;p<0,01].
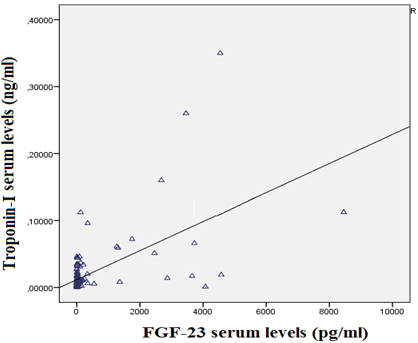
Fig. 3 - Correlation of sFGF-23 with Tr-I in CKD patients
In the patients with elevated CBP (> 120/80 mm. Hg.) and in normal CBP (90-120 / 70-79mm. Hg.) mean levels of sFGF-23 were about the same [629+118 and 489+85], indicating about independent from the CBP effect of sFGF-23 on myocardium. In the same time levels of Tr-I correlated with LVMI [r = 0,544; p<0,01], CMR [r=0,449;p<0,01], BSE[r= - 0,514;p<0,01], DDLV [r= 0,492; p<0,01], kidney disease duration in months [r = 0,468; p <0,05], presence of arrhythmias in ECG [r=0,445;p<0,05], CBP [r=0,534;p<0,01]. Between sKlotho levels and Tr-I [r= - 0,537; p<0,01], PVW [r=-0,647;p<0,01], DHC [r=- 0,612; p<0,01], LVMI [r = - 0,539; p <0,01], CMR [r=- 0,528;p<0,01] we found negative associations.
According to multivariate analysis, Tr-I serum levels were associated with decreased of sKlotho (p=0,0004), increased of sFGF-23(p=0,002) and increased of CBP (p=0,0012).
Conclusion: In our study minimally elevated Tr-I serum levels were associated with decreased sKlotho and elevated sFGF-23 in CKD patients without sCVD.
Discussion: In our study, rising of sFGF-23 in 110 CKD patients without clinical symptoms of CC was associated with an increase in serum Tr-I. Association between sFGF-23 and Tr-I was not hunted from the traditional risk factors. It was also repeatedly demonstrated [14,15,16] that traditional CC risk factors did not correlate with the level of troponins indicates that atherosclerosis is not cause of troponins increasing in patients with CKD.
It was found out [17] an increase in Tr- T level was not connected with ischemic cardiac disease (ICD) despite of 33% ICD patients in the study. According to Smith K. et al. [18] tropnins were higher despite the absence of ICD history in the patients.
All this findings makes us to look for the cause of some elevated troponins in patients with CKD among uremic factors.
It has been shown that elevated sFGF-23 is early marker of CVD in CKD and associated with high mortality and FGF-23 is considered now as a new uremic toxin instead of PTH because firstly of its pathologic action on heart but exactly ways of sFGF-23-effects is not installed yet. Our findings indicate on association between sFGF-23 and Tr-I, which may be a result of sFGF-23 cardiotoxic effect on the myocardium, leading to the increase of serum Tr-I.
At the same time according to our date increasing sFGF-23 may be secondary to the Klotho deficiency. Our findings demonstrated an inverse relationship between of Klotho levels and serum detectable Tr-I.
Based on the identified results and the literature date sKlotho may consider as a main therapeutic option in the near future.
Conflict of interest statement None declared. Acknowledgements This work was supported by the Russian Science Foundation (grant № 14-15-00947 2014)References
- Couser WG.,Remuzzi G.,Mendis S.et al. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases// Kidney int. 2011. Vol. 80. No 12. P. 1258-1270
- Lu KC., Wu CC., Yen JF., et al. Vascular calcification and Renal Bone Disorders// Scientific World Journal 2014. Published online 2014 Jul 17. doi: 10.1155/2014/637065
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evalution, prevention, and treatment of chronic kidney disease -mineral and bone disorder (CKD-MBD)//Kidney Int. 2009. Vol. 76. Suppl.113. P. 1-130
- Hu M.C., Shiizaki K., Kuro-o M. et al. Fibroblast Growth Factor 23 and Klotho: Physiology and Pathophysiology of an Endocrine Network of Mineral Metabolism// Annu Rev Physiol. 2013. No 75. P. 503–533. doi: 10.1146/annurev-physiol-030212-183727
- Scialla J.J., Xie H., Rahman M. et al. Fibroblast Growth Factor-23 and Cardiovascular Events in CKD, the Chronic Renal Insufficiency Cohort (CRIC) Study Investigators// J Am Soc Nephrol. 2014. Vol. 25. No2. P. 349–360. doi: 10.1681/ASN.2013050465
- Milovanova L., Milovanov Y., Plotnikova A. Phosphorus and Calcium Metabolism Disorders Assosiated with Chronic Kidney Disease Stage III -IV (Systematic Rewiew and Meta-Analysis)// In: Chronic Kidney Disease and renal Transplantation.-Groatia.: INTECH, 2012. P. 95-118
- Hu MC., Kuro-o M., Moe OW. et al. Klotho and Chronic Kidney Disease// Contrib Nephrol. 2013. Vol. 180. P.47–63.
- Hu MC., Kuro-o M., Moe OW., Klotho and Chronic Kidney Disease //Contrib Nephrol. 2013. Vol. 180. P. 47–63.
- Kuro-o M. Klotho in chronic kidney disease—What's new?// Nephrology Dialysis Transplant 2009. Vol. 24. No 6. P. 1705-1708
- Hu MC., Shi M., Zhang J. et al. Klotho deficiency causes vascular calcification in chronic kidney disease// Am. J. Soc. Nephrol. 2011. Vol. 22. No 1. P. 124-136
- Hu MC., Kuro-o M., Moe OW. RENAL AND EXTRA-RENAL ACTIONS OF KLOTHO// Semin Nephrol. 2013. Vol. 33. No 2. P. 118–129
- Milovanova L.Y., Milovanov Y.S., Kozlovskaya L.V. Nephro-cardioprotective role of the circulating forms of the KLOTHO protein in chronic kidney disease// Clinical Nephrology 2013. Vol.3. P. 7-10
- Chen S., Huang H., Wu B. et al. Cardiac Troponin I in Non- Acute Coronary Syndrome Patients with Chronic Kidney Disease// PLoS One. 2013. Vol. 8. No 12. doi: 10.1371/journal.pone.0082752
- Abbas NA, John RI, Webb MC, et al. Cardiac troponins and renal function in nondialysis patients with chronic kidney disease// Clin Chem. 2005. Vol. 51. No 11. P. 2059–2066.
- Wang AY, Lam CW, Wang M, et al. Prognostic value of cardiac troponin T is independent of inflammation, residual renal function, and cardiac hypertrophy and dysfunction in peritoneal dialysis patients// Clin Chem. 2007. Vol.53. No 5. P. 882–889.
- deFilippi C, Wasserman S, Rosanio S, et al. Cardiac troponin T and C-reactive protein for predicting prognosis, coronary atherosclerosis, and cardiomyopathy in patients undergoing long-term hemodialysis// JAMA. 2003. Vol. 290. No 3. P. 353–359.
- McMurray JJ, Uno H, Jarolim P, et al. Predictors of fatal and nonfatal cardiovascular events in patients with type 2 diabetes mellitus, chronic kidney disease, and anemia: an analysis of the Trial to Reduce cardiovascular Events with Aranesp (darbepoetin-alfa) Therapy (TREAT) //Am Heart J. 2011. Vol. 162. No 4. P. 748–755. e743.
- Smith K., deFilippi C., Isakov T. et al. Fibroblast Growth Factor 23, High-Sensitivity Cardiac Troponin, and Left Ventricular Hypertrophy in CKD//Am J Kidney Dis. 2013. Vol. 61. No 1. P. 67–73. doi: 10.1053/j.ajkd.2012.06.022s